

Enhanced recovery following hip and knee arthroplasty: a systematic review of cost-effectiveness evidence
- PMID: 31948987
- PMCID: PMC7044879
- DOI: 10.1136/bmjopen-2019-032204
Enhanced recovery following hip and knee arthroplasty: a systematic review of cost-effectiveness evidence
Abstract
Objectives: To assess cost-effectiveness of enhanced recovery pathways following total hip and knee arthroplasties. Secondary objectives were to report on quality of studies and identify research gaps for future work.
Design: Systematic review of cost-utility analyses.
Data sources: Ovid MEDLINE, Embase, the National Health Service Economic Evaluations Database and EconLit, January 2000 to August 2019.
Eligibility criteria: English-language peer-reviewed cost-utility analyses of enhanced recovery pathways, or components of one, compared with usual care, in patients having total hip or knee arthroplasties for osteoarthritis.
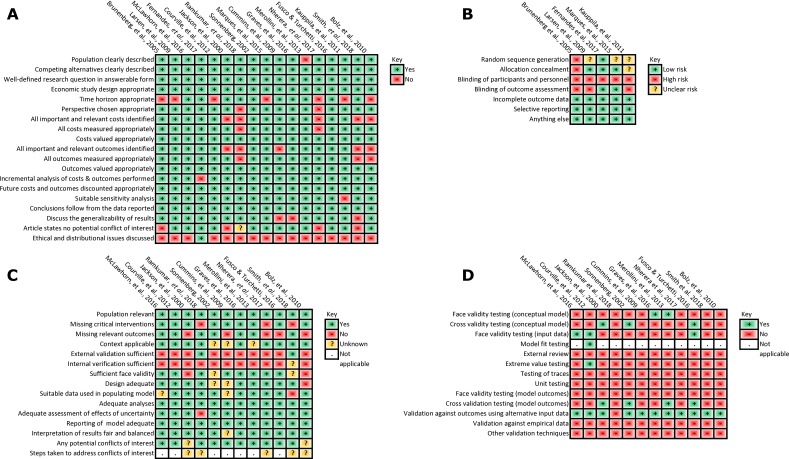
Data extraction and synthesis: Data extracted by three reviewers with disagreements resolved by a fourth. Study quality assessed using the Consensus on Health Economic Criteria list, the International Society for Pharmacoeconomics and Outcomes Research and Assessment of the Validation Status of Health-Economic decision models tools; for trial-based studies the Cochrane Collaboration's tool to assess risk of bias. No quantitative synthesis was undertaken.
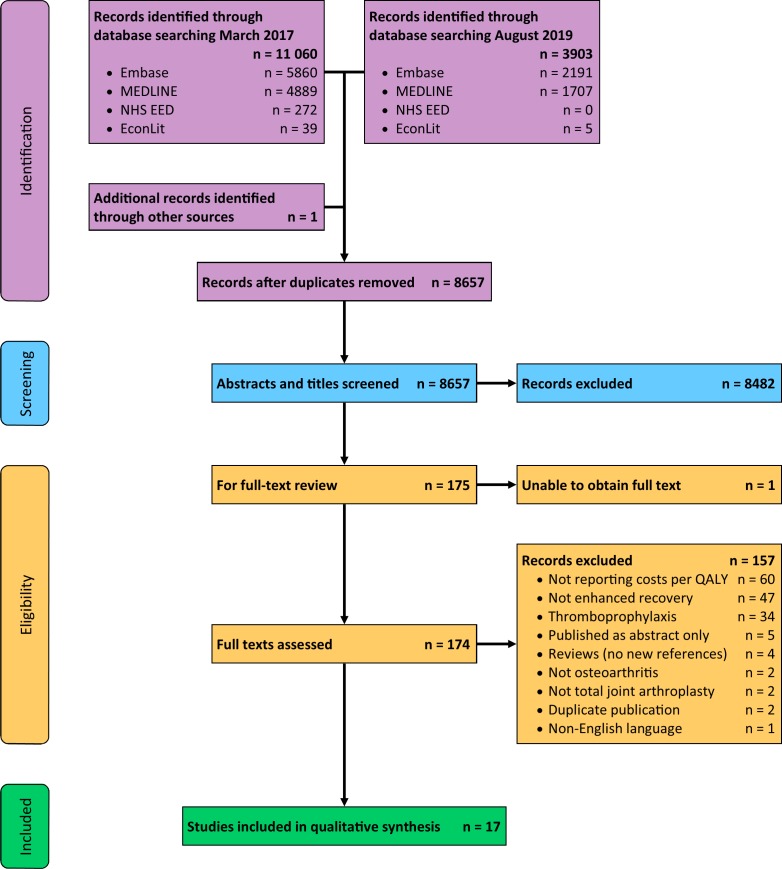
Results: We identified 17 studies: five trial-based and 12 model-based studies. Two analyses evaluated entire enhanced recovery pathways and reported them to be cost-effective compared with usual care. Ten pathway components were more effective and cost-saving compared with usual care, three were cost-effective, and two were not cost-effective. We had concerns around risk of bias for all included studies, particularly regarding the short time horizon of the trials and lack of reporting of model validation.
Conclusions: Consistent results supported enhanced recovery pathways as a whole, prophylactic systemic antibiotics, antibiotic-impregnated cement and conventional ventilation for infection prevention. No other interventions were subject of more than one study. We found ample scope for future cost-effectiveness studies, particularly analyses of entire recovery pathways and comparison of incremental changes within pathways. A key limitation is that standard practices have changed over the period covered by the included studies.
Prospero registration number: CRD42017059473.
Keywords: cost-effectiveness; economic evaluation; hip replacement; knee replacement; osteoarthritis; systematic review.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Cost-effectiveness of enhanced recovery in hip and knee replacement: a systematic review protocol.BMJ Open. 2018 Mar 14;8(3):e019740. doi: 10.1136/bmjopen-2017-019740. BMJ Open. 2018. PMID: 29540418 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
The Arthroplasty Candidacy Help Engine tool to select candidates for hip and knee replacement surgery: development and economic modelling.Health Technol Assess. 2019 Jun;23(32):1-216. doi: 10.3310/hta23320. Health Technol Assess. 2019. PMID: 31287051 Free PMC article.
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Better post-operative prediction and management of chronic pain in adults after total knee replacement: the multidisciplinary STAR research programme including RCT.Southampton (UK): National Institute for Health and Care Research; 2023 Jun. Southampton (UK): National Institute for Health and Care Research; 2023 Jun. PMID: 37494508 Free Books & Documents. Review.
Cited by
-
Cost-Effectiveness of GaitSmart and an Artificial Intelligence Solution for Rehabilitation of Patients Undergoing Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in Older Population in the United Kingdom.Geriatrics (Basel). 2024 Oct 5;9(5):129. doi: 10.3390/geriatrics9050129. Geriatrics (Basel). 2024. PMID: 39451861 Free PMC article.
-
[Enhanced recovery after surgery-Does the ERAS concept keep its promises].Chirurg. 2021 May;92(5):405-420. doi: 10.1007/s00104-020-01328-y. Epub 2021 Jan 22. Chirurg. 2021. PMID: 33481060 Review. German.
-
Trends and Themes in the Study of Value in Orthopedic Surgery: A Systematic Review.HSS J. 2025 Feb;21(1):93-101. doi: 10.1177/15563316231204040. Epub 2023 Oct 24. HSS J. 2025. PMID: 39846060 Free PMC article. Review.
-
Systemic medical complications following joint replacement: a review of the evidence.Ann R Coll Surg Engl. 2023 Mar;105(3):191-195. doi: 10.1308/rcsann.2022.0012. Epub 2022 Jun 10. Ann R Coll Surg Engl. 2023. PMID: 35686748 Free PMC article. Review.
-
A comparison between barbed suture and conventional suture in total knee arthroplasty: a systematic review and meta-analysis.Arthroplasty. 2020 Mar 27;2(1):8. doi: 10.1186/s42836-020-00028-6. Arthroplasty. 2020. PMID: 35236431 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical