

Culture of pulmonary artery endothelial cells from pulmonary artery catheter balloon tips: considerations for use in pulmonary vascular disease
- PMID: 31949110
- PMCID: PMC7147989
- DOI: 10.1183/13993003.01313-2019
Culture of pulmonary artery endothelial cells from pulmonary artery catheter balloon tips: considerations for use in pulmonary vascular disease
Abstract
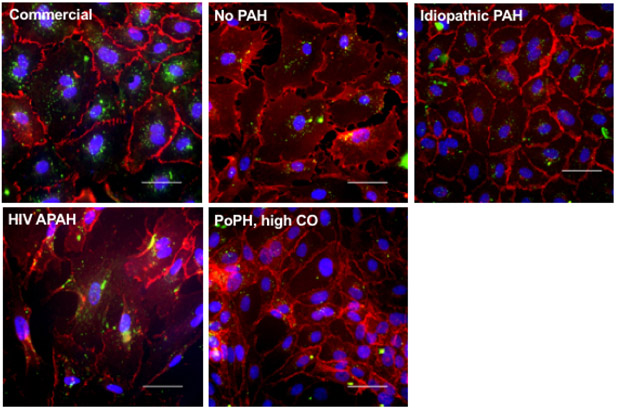
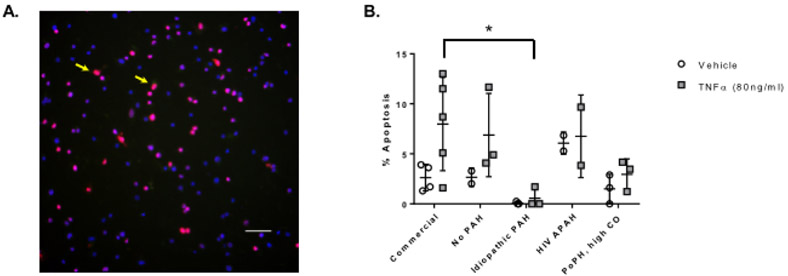
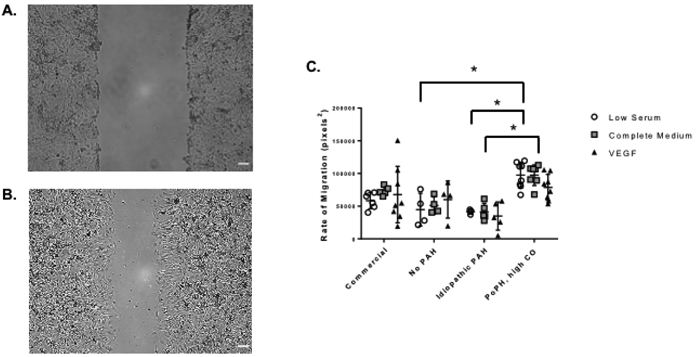
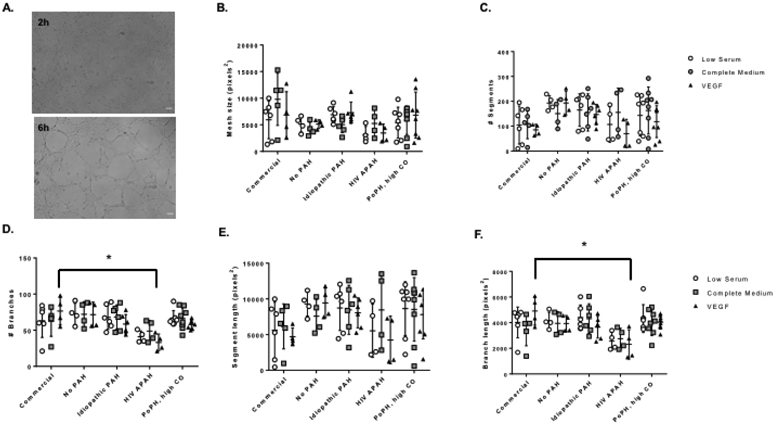
Endothelial dysfunction is a hallmark of pulmonary arterial hypertension (PAH) but there are no established methods to study pulmonary artery endothelial cells (PAECs) from living patients. We sought to culture PAECs from pulmonary artery catheter (PAC) balloons used during right-heart catheterisation (RHC) to characterise successful culture attempts and to describe PAEC behaviour.PAECs were grown in primary culture to confluence and endothelial cell phenotype was confirmed. Standard assays for apoptosis, migration and tube formation were performed between passages three to eight. We collected 49 PAC tips from 45 subjects with successful PAEC culture from 19 balloons (39%).There were no differences in subject demographic details or RHC procedural details in successful versus unsuccessful attempts. However, for subjects who met haemodynamic criteria for PAH, there was a higher but nonsignificant (p=0.10) proportion amongst successful attempts (10 out of 19, 53%) versus unsuccessful attempts (nine out of 30, 30%). A successful culture was more likely in subjects with a lower cardiac index (p=0.03) and higher pulmonary vascular resistance (p=0.04). PAECs from a subject with idiopathic PAH were apoptosis resistant compared to commercial PAECs (p=0.04) and had reduced migration compared to PAECs from a subject with portopulmonary hypertension with high cardiac output (p=0.01). PAECs from a subject with HIV-associated PAH formed fewer (p=0.01) and shorter (p=0.02) vessel networks compared to commercial PAECs.Sustained culture and characterisation of PAECs from RHC balloons is feasible, especially in PAH with high haemodynamic burden. This technique may provide insight into endothelial dysfunction during PAH pathogenesis.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: C.E. Ventetuolo reports grants from National Institutes of Health (R01 HL141268 and P20GM103652), during the conduct of the study; institutional grants from United Therapeutics and Eiger; personal fees from Acceleron Pharma, outside the submitted work; and her spouse was a recent employee of CVS Health. Conflict of interest: J.M. Aliotta has nothing to disclose. Conflict of interest: J. Braza has nothing to disclose. Conflict of interest: H. Chichger has nothing to disclose. Conflict of interest: M. Dooner has nothing to disclose. Conflict of interest: D. McGuirl has nothing to disclose. Conflict of interest: C.J. Mullin has nothing to disclose. Conflict of interest: J. Newton has nothing to disclose. Conflict of interest: M. Pereira has nothing to disclose. Conflict of interest: A. Princiotto has nothing to disclose. Conflict of interest: P.J. Quesenberry has nothing to disclose. Conflict of interest: T. Walsh has nothing to disclose. Conflict of interest: M. Whittenhall has nothing to disclose. Conflict of interest: J.R. Klinger has nothing to disclose. Conflict of interest: E.O. Harrington has nothing to disclose.
Figures
Comment in
-
Tips for success in pulmonary hypertension treatment: progress in isolating endothelial cells from pulmonary artery catheters.Eur Respir J. 2020 Mar 20;55(3):2000122. doi: 10.1183/13993003.00122-2020. Print 2020 Mar. Eur Respir J. 2020. PMID: 32198271 Free PMC article. No abstract available.
References
-
- Budhiraja R, Tuder RM, Hassoun PM. Endothelial dysfunction in pulmonary hypertension. Circulation 2004; 109: 159–165. - PubMed
-
- Gu M, Shao NY, Sa S, Li D, Termglinchan V, Ameen M, Karakikes I, Sosa G, Grubert F, Lee J, Cao A, Taylor S, Ma Y, Zhao Z, Chappell J, Hamid R, Austin ED, Gold JD, Wu JC, Snyder MP, Rabinovitch M. Patient-specific iPSC-derived endothelial cells uncover pathways that protect against pulmonary hypertension in BMPR2 mutation carriers. Cell Stem Cell 2017; 20: 490–504.e495. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous