

Chronotherapy of Non-Steroidal Anti-Inflammatory Drugs May Enhance Postoperative Recovery
- PMID: 31949183
- PMCID: PMC6965200
- DOI: 10.1038/s41598-019-57215-y
Chronotherapy of Non-Steroidal Anti-Inflammatory Drugs May Enhance Postoperative Recovery
Abstract
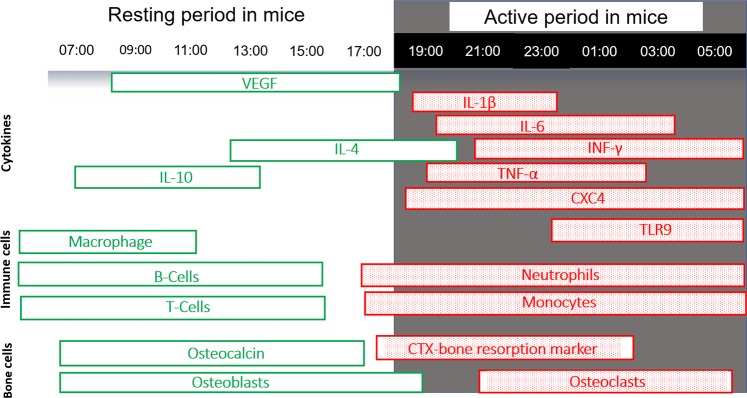
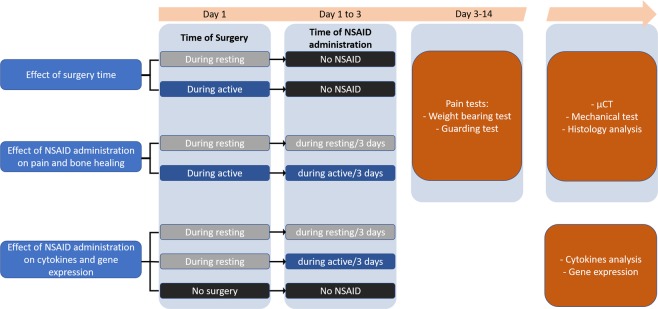
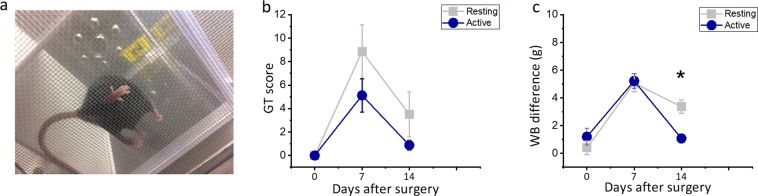
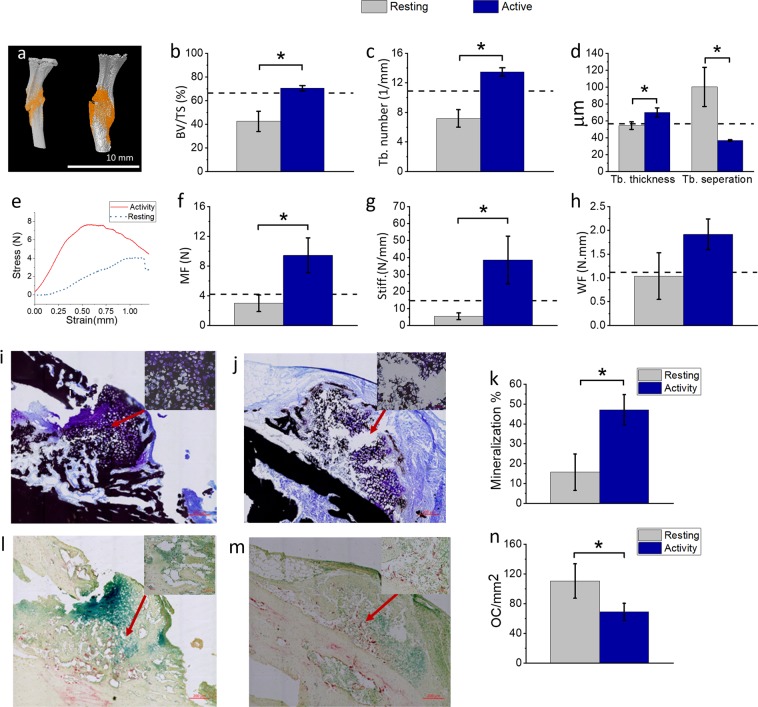
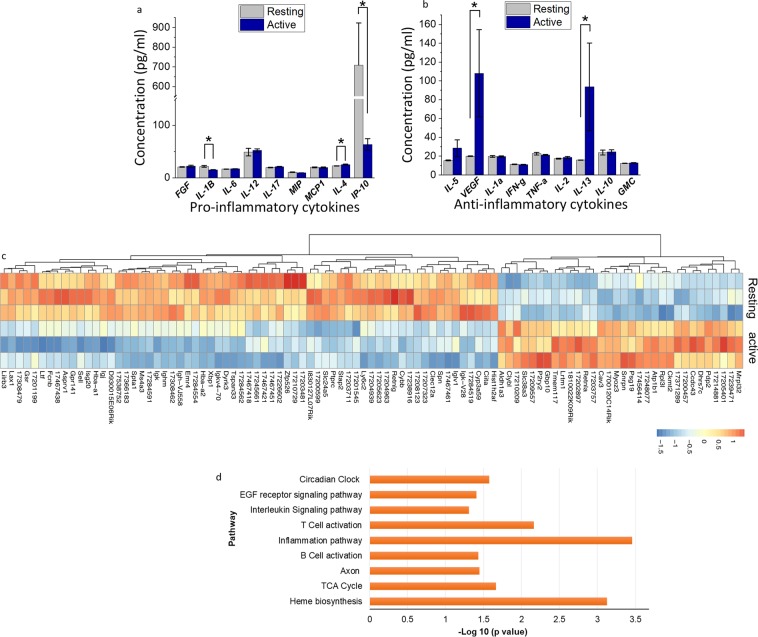
Postoperative pain relief is crucial for full recovery. With the ongoing opioid epidemic and the insufficient effect of acetaminophen on severe pain; non-steroidal anti-inflammatory drugs (NSAIDs) are heavily used to alleviate this pain. However, NSAIDs are known to inhibit postoperative healing of connective tissues by inhibiting prostaglandin signaling. Pain intensity, inflammatory mediators associated with wound healing and the pharmacological action of NSAIDs vary throughout the day due to the circadian rhythm regulated by the clock genes. According to this rhythm, most of wound healing mediators and connective tissue formation occurs during the resting phase, while pain, inflammation and tissue resorption occur during the active period of the day. Here we show, in a murine tibia fracture surgical model, that NSAIDs are most effective in managing postoperative pain, healing and recovery when drug administration is limited to the active phase of the circadian rhythm. Limiting NSAID treatment to the active phase of the circadian rhythm resulted in overexpression of circadian clock genes, such as Period 2 (Per2) at the healing callus, and increased serum levels of anti-inflammatory cytokines interleukin-13 (IL-13), interleukin-4 (IL-4) and vascular endothelial growth factor. By contrast, NSAID administration during the resting phase resulted in severe bone healing impairment.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
