

MiT family translocation renal cell carcinoma after malignant infantile osteopetrosis in childhood: a case report
- PMID: 31949762
- PMCID: PMC6962853
MiT family translocation renal cell carcinoma after malignant infantile osteopetrosis in childhood: a case report
Abstract
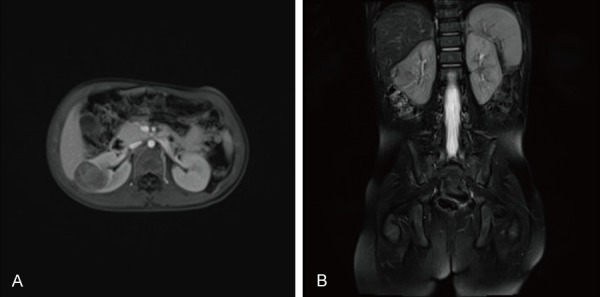
Malignant infantile osteopetrosis (MIOP) is a rare inherited bone metabolism disorder characterized by increased bone mineral density (BMD) and abnormal hematopoiesis. Hematopoietic stem cell transplantation (HSCT) is currently the only curative therapy for MIOP. However, a higher risk of secondary malignancy occurs in children previously exposed to cytotoxic drugs. Here we report a rare case of a 3-year-old female patient with MiT family translocation renal cell carcinoma (MiTF tRCC), who is a survivor of HSCT for MIOP 2 years earlier. The patient had a complete resection of the tumor. Microscopically, we detected diffusely and papillary-like arranged tumor cells whose cytoplasm was bright and clear. Immunohistochemistry showed tumor cells diffusely expressed TFE3, and fluorescence in situ hybridization (FISH) demonstrated disruption of the TFE3 locus, confirming the diagnosis of Xp11 translocation RCC, the subtype of MiTF tRCC. This case supports the view that chemotherapy exposure is a risk factor for MiTF tRCC and indicates the possible association of HSCT with MiTF tRCC.
Keywords: Malignant infantile osteopetrosis; MiT family translocation renal cell carcinoma; Xp11 translocation renal cell carcinoma; chemotherapy; hematopoietic stem cell transplantation.
IJCEP Copyright © 2018.
Conflict of interest statement
None.
Figures




References
-
- Sobacchi C, Schulz A, Coxon FP, Villa A, Helfrich MH. Osteopetrosis: genetics, treatment and new insights into osteoclast function. Nat Rev Endocrinol. 2013;9:522–536. - PubMed
-
- Eapen M, Davies SM, Ramsay NK, Orchard PJ. Hematopoietic stem cell transplantation for infantile osteopetrosis. Blood. 2015;2:270–276. - PubMed
-
- Srigley JR, Delahunt B, Eble JN, Egevad L, Epstein JI, Grignon D, Hes O, Moch H, Montironi R, Tickoo SK, Zhou M, Argani P. The international society of urological pathology (ISUP) vancouver classification of renal neoplasia. Am J Surg Pathol. 2013;37:1469–1489. - PubMed
Publication types
LinkOut - more resources
Full Text Sources