

Atherosclerotic Cardiovascular Disease Risk Profile of Tenofovir Alafenamide Versus Tenofovir Disoproxil Fumarate
- PMID: 31950070
- PMCID: PMC6954396
- DOI: 10.1093/ofid/ofz472
Atherosclerotic Cardiovascular Disease Risk Profile of Tenofovir Alafenamide Versus Tenofovir Disoproxil Fumarate
Abstract
Background: In human immunodeficiency virus (HIV) treatment, tenofovir alafenamide (TAF) is associated with greater increases in all fasting cholesterol subgroups compared with tenofovir disoproxil fumarate (TDF). Because lipid abnormalities may contribute to cardiovascular morbidity and mortality, cardiovascular risk assessment is integral to routine HIV care. This post hoc study evaluates the impact of lipid changes on predicted atherosclerotic cardiovascular disease (ASCVD) risk and statin eligibility in treatment-naive adults living with HIV treated with TAF or TDF.
Methods: Participants (N = 1744) were randomized (1:1) to initiate TAF or TDF, each coformulated with elvitegravir/cobicistat/emtricitabine (studies GS-US-292-0104 and GS-US-292-0111). Eligibility for statin therapy and estimated 10-year ASCVD risk among adults aged 40-79 years treated with TAF or TDF for 96 weeks (W96) were analyzed based on American College of Cardiology/American Heart Association Pooled Cohort Equations. Categorical shifts in 10-year ASCVD risk from <7.5% to ≥7.5% by W96 on TAF versus TDF were calculated.
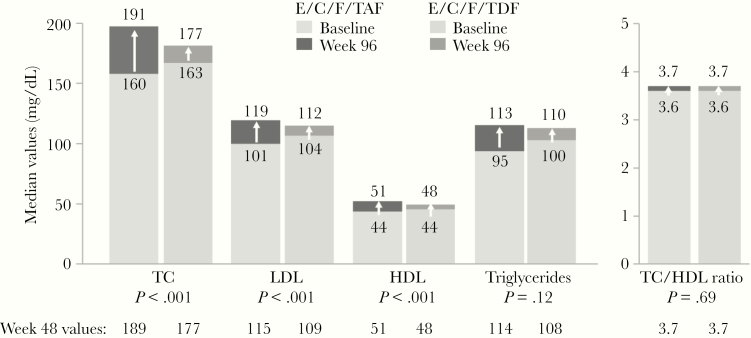
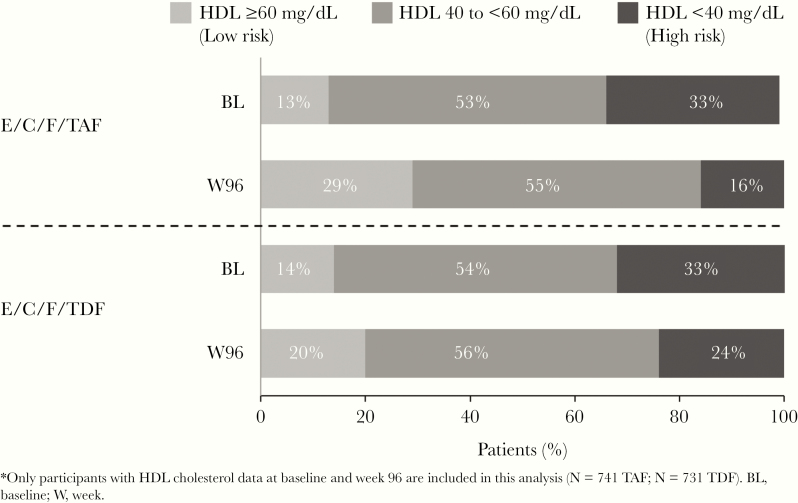
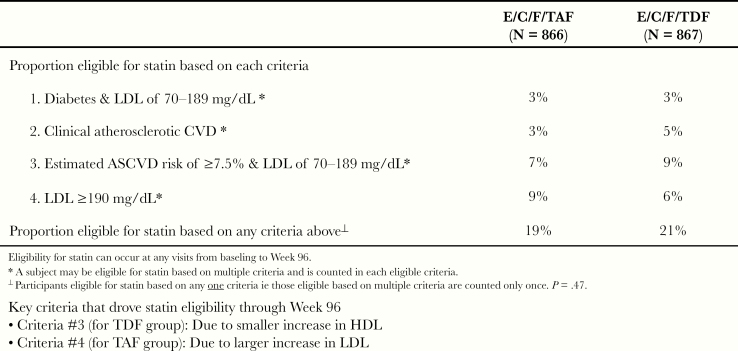
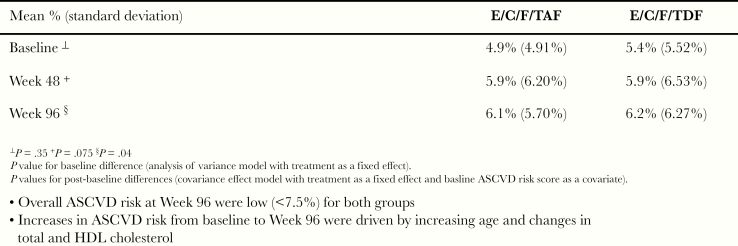
Results: Participants initiating TAF versus TDF in the overall study population showed small but significant increases in median fasting lipid parameters at W96, including total cholesterol (191 vs 177 mg/dL; P < .001), low-density lipoprotein ([LDL] 119 vs 112 mg/dL; P < .001), and high-density lipoprotein ([HDL] 51 vs 48 mg/dL; P < .001), respectively. At baseline, 18% and 23% on TAF versus TDF had a 10-year ASCVD risk score ≥7.5%, with mean risk scores low overall for TAF versus TDF at baseline (4.9% vs 5.4%; P = .35) and W96 (6.1% vs 6.2%; P = .04). Increases in ASCVD risk from baseline to W96 were driven by both increasing age and changes in total cholesterol (TC) and HDL cholesterol. At W96, TC/HDL ratios (median) were 3.7 for both groups (P = .69). There was no difference between shifts in categorical risk for TAF versus TDF (9% vs 5%; P = .19). Eligibility for high-intensity statin therapy were similar for TAF versus TDF groups (19% vs 21%; P = .47).
Conclusions: Lipid changes with TAF as part of coformulated regimens do not substantively affect CVD risk profiles compared with TDF.
Keywords: HIV; atherosclerosis; cardiovascular disease; tenofovir alafenamide; tenofovir disoproxil fumarate.
© The Author(s) 2019. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures

References
-
- Kaplan-Lewis E, Aberg JA, Lee M. Aging with HIV in the ART era. Semin Diagn Pathol 2017; 34:384–97. - PubMed
-
- Tarr PE, Ledergerber B, Calmy A, et al. . Subclinical coronary artery disease in Swiss HIV-positive and HIV-negative persons. European Heart Journal 2018;39:2147–2154. - PubMed
-
- Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. . 2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014; 129(25 Suppl 2):S49–73. - PubMed
