

Fulminant corticobasal degeneration: a distinct variant with predominant neuronal tau aggregates
- PMID: 31950334
- PMCID: PMC7096362
- DOI: 10.1007/s00401-019-02119-4
Fulminant corticobasal degeneration: a distinct variant with predominant neuronal tau aggregates
Abstract
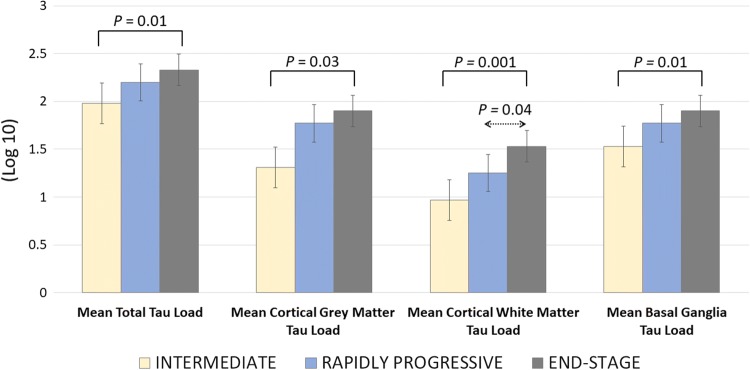
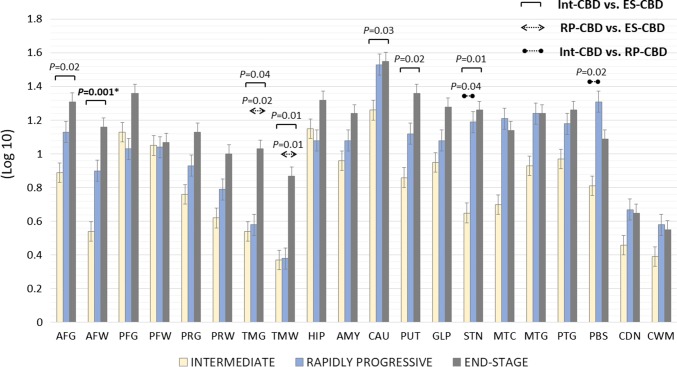
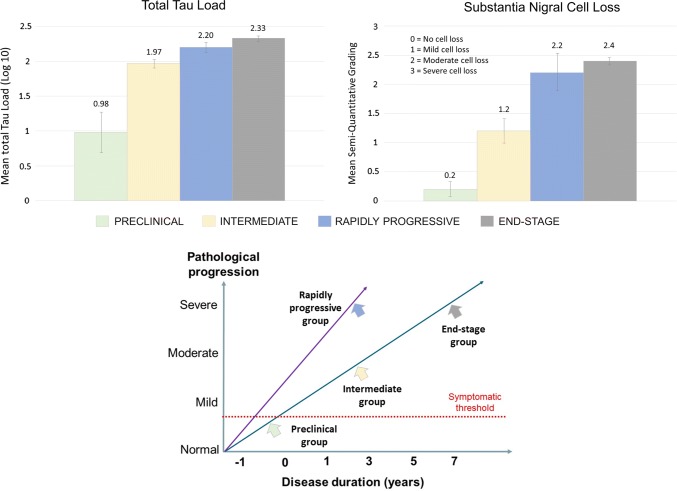
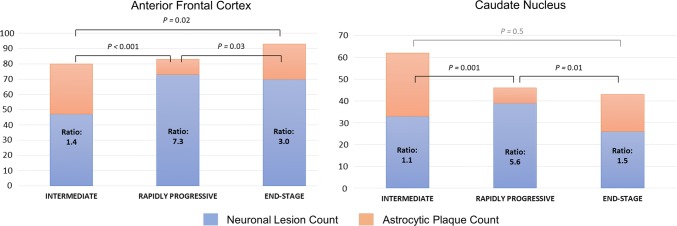
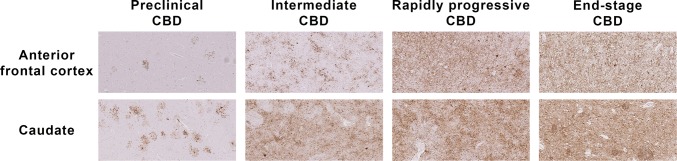
Corticobasal degeneration typically progresses gradually over 5-7 years from onset till death. Fulminant corticobasal degeneration cases with a rapidly progressive course were rarely reported (RP-CBD). This study aimed to investigate their neuropathological characteristics. Of the 124 autopsy-confirmed corticobasal degeneration cases collected from 14 centres, we identified 6 RP-CBD cases (4.8%) who died of advanced disease within 3 years of onset. These RP-CBD cases had different clinical phenotypes including rapid global cognitive decline (N = 2), corticobasal syndrome (N = 2) and Richardson's syndrome (N = 2). We also studied four corticobasal degeneration cases with an average disease duration of 3 years or less, who died of another unrelated illness (Intermediate-CBD). Finally, we selected 12 age-matched corticobasal degeneration cases out of a cohort of 110, who had a typical gradually progressive course and reached advanced clinical stage (End-stage-CBD). Quantitative analysis showed high overall tau burden (p = 0.2) and severe nigral cell loss (p = 0.47) in both the RP-CBD and End-stage-CBD groups consistent with advanced pathological changes, while the Intermediate-CBD group (mean disease duration = 3 years) had milder changes than End-stage-CBD (p < 0.05). These findings indicated that RP-CBD cases had already developed advanced pathological changes as those observed in End-stage-CBD cases (mean disease duration = 6.7 years), but within a significantly shorter duration (2.5 years; p < 0.001). Subgroup analysis was performed to investigate the cellular patterns of tau aggregates in the anterior frontal cortex and caudate by comparing neuronal-to-astrocytic plaque ratios between six RP-CBD cases, four Intermediate-CBD and 12 age-matched End-stage-CBD. Neuronal-to-astrocytic plaque ratios of Intermediate-CBD and End-stage-CBD, but not RP-CBD, positively correlated with disease duration in both the anterior frontal cortex and caudate (p = 0.02). In contrast to the predominance of astrocytic plaques we previously reported in preclinical asymptomatic corticobasal degeneration cases, neuronal tau aggregates predominated in RP-CBD exceeding those in Intermediate-CBD (anterior frontal cortex: p < 0.001, caudate: p = 0.001) and End-stage-CBD (anterior frontal cortex: p = 0.03, caudate: p = 0.01) as demonstrated by its higher neuronal-to-astrocytic plaque ratios in both anterior frontal cortex and caudate. We did not identify any difference in age at onset, any pathogenic tau mutation or concomitant pathologies that could have contributed to the rapid progression of these RP-CBD cases. Mild TDP-43 pathology was observed in three RP-CBD cases. All RP-CBD cases were men. The MAPT H2 haplotype, known to be protective, was identified in one RP-CBD case (17%) and 8 of the matched End-stage-CBD cases (67%). We conclude that RP-CBD is a distinct aggressive variant of corticobasal degeneration with characteristic neuropathological substrates resulting in a fulminant disease process as evident both clinically and pathologically. Biological factors such as genetic modifiers likely play a pivotal role in the RP-CBD variant and should be the subject of future research.
Keywords: Astrocytic plaques; Corticobasal degeneration; Neurofibrillary tangles; Progressive supranuclear palsy; Tau.
Conflict of interest statement
H.L. K.D., K.Y.M, R.S, T.B, S.W., N.S-S, R. dS., H.R.M, J.H., T.T.W., J.L.H., T.R. receive research grant from Karin & Sten Mortstedt CBD Solutions. EG received a grant from the Fundació Marató de TV3 (Grant number: 20141610). GMH is supported by an NHMRC Senior Principal Research Fellowship. H.R.M. receives research grant from the PSP Association. E.J. is supported by a MRC Fellowship. M.J.E. receives funding from Cancer Research UK Accelerator Grant (C1 15121 A 20256). Other authors report no conflict of interest.
Figures
References
-
- Ahmed Z, Cooper J, Murray TK, Garn K, McNaughton E, Clarke H, et al. A novel in vivo model of tau propagation with rapid and progressive neurofibrillary tangle pathology: the pattern of spread is determined by connectivity, not proximity. Acta Neuropathol. 2014;127:667–683. doi: 10.1007/s00401-014-1254-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- G0701075/MRC_/Medical Research Council/United Kingdom
- G0502157/MRC_/Medical Research Council/United Kingdom
- G0900580/MRC_/Medical Research Council/United Kingdom
- G0400074/MRC_/Medical Research Council/United Kingdom
- MR/N026004/1/MRC_/Medical Research Council/United Kingdom
- G0901254/MRC_/Medical Research Council/United Kingdom
- MR/S000992/1/MRC_/Medical Research Council/United Kingdom
- MR/L501542/1/MRC_/Medical Research Council/United Kingdom
- MR/K01417X/1/MRC_/Medical Research Council/United Kingdom
- G-0907/PUK_/Parkinson's UK/United Kingdom
- MC_PC_14095/MRC_/Medical Research Council/United Kingdom
- G0900652/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
