

Immune cell phenotyping in low blood volumes for assessment of cardiovascular disease risk, development, and progression: a pilot study
- PMID: 31952533
- PMCID: PMC6966880
- DOI: 10.1186/s12967-020-02207-0
Immune cell phenotyping in low blood volumes for assessment of cardiovascular disease risk, development, and progression: a pilot study
Abstract
Background: Cardiovascular disease (CVD) is the leading cause of death in the world. Given the role of immune cells in atherosclerosis development and progression, effective methods for characterizing immune cell populations are needed, particularly among populations disproportionately at risk for CVD.
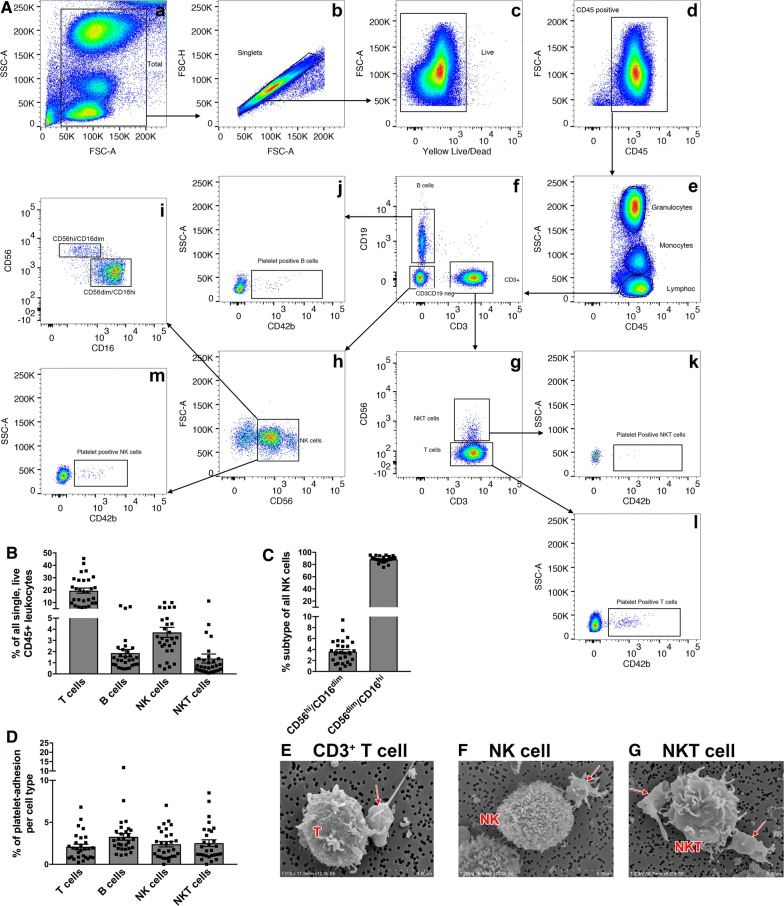
Results: By using a variety of antibodies combined in one staining protocol, we were able to identify granulocyte, lymphocyte, and monocyte sub-populations by CD-antigen expression from 500 µl of whole blood, enabling a more extensive comparison than what is possible with a complete blood count and differential (CBC). The flow cytometry panel was established and tested in a total of 29 healthy men and women. As a proof of principle, these 29 samples were split by their race/ethnicity: African-Americans (AA) (N = 14) and Caucasians (N = 15). We found in accordance with the literature that AA had fewer granulocytes and more lymphocytes when compared to Caucasians, though the proportion of total monocytes was similar in both groups. Several new differences between AA and Caucasians were noted that had not been previously described. For example, AA had a greater proportion of platelet adhesion on non-classical monocytes when compared to Caucasians, a cell-to-cell interaction described as crucially important in CVD. We also examined our flow panel in a clinical population of AA women with known CVD risk factors (N = 20). Several of the flow cytometry parameters that cannot be measured with the CBC displayed correlations with clinical CVD risk markers. For instance, Framingham Risk Score (FRS) calculated for each participant correlated with immune cell platelet aggregates (PA) (e.g. T cell PA β = 0.59, p = 0.03 or non-classical monocyte PA β = 0.54, p = 0.02) after adjustment for body mass index (BMI).
Conclusion: A flow cytometry panel identified differences in granulocytes, monocytes, and lymphocytes between AA and Caucasians which may contribute to increased CVD risk in AA. Moreover, this flow panel identifies immune cell sub-populations and platelet aggregates associated with CVD risk. This flow cytometry panel may serve as an effective method for phenotyping immune cell populations involved in the development and progression of CVD.
Keywords: Blood cell composition; Cardiovascular disease; Flow cytometry; Health disparities; Platelet adhesion.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Carnethon MR, Pu J, Howard G, Albert MA, Anderson CAM, Bertoni AG, Mujahid MS, Palaniappan L, Taylor HA, Jr, Willis M, et al. Cardiovascular Health in African Americans: a Scientific Statement From the American Heart Association. Circulation. 2017;136:e393–e423. doi: 10.1161/CIR.0000000000000534. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
