

Ablation of atrial fibrillation during coronary artery bypass grafting: Late outcomes in a Medicare population
- PMID: 31952824
- PMCID: PMC10108849
- DOI: 10.1016/j.jtcvs.2019.10.159
Ablation of atrial fibrillation during coronary artery bypass grafting: Late outcomes in a Medicare population
Abstract
Background: This study compares outcomes of patients with preoperative atrial fibrillation undergoing coronary artery bypass grafting (CABG) with or without concomitant atrial fibrillation ablation in a nationally representative Medicare cohort.
Objectives: This study examined early and late outcomes in CABG patients with a preoperative history of atrial fibrillation to determine the correlation between surgical atrial fibrillation ablation to mortality and stroke or systemic embolization.
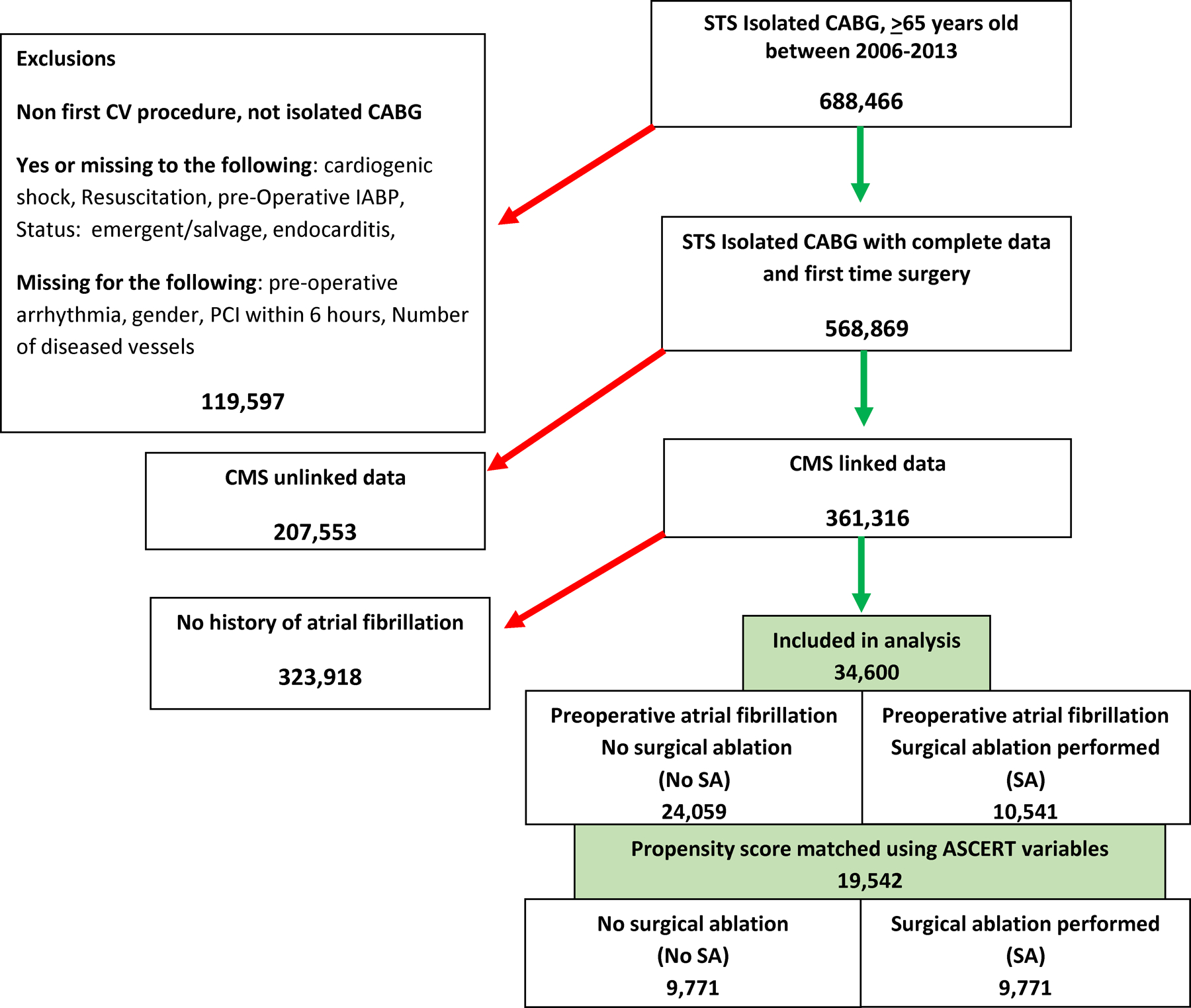
Methods: In the Medicare-linked Society of Thoracic Surgeons database, 361,138 patients underwent isolated CABG from 2006 to 2013; 34,600 (9.6%) had preoperative atrial fibrillation; 10,541 (30.5%) were treated with surgical ablation (ablation group), and 23,059 were not (no ablation group). Propensity score matching was performed using a hierarchical mixed model. Long-term survival was summarized using Kaplan-Meier curves and Cox regression models with robust variance estimation. The stroke or systemic embolization incidence was modeled using the Fine-Gray model. Median follow-up was 4 years.
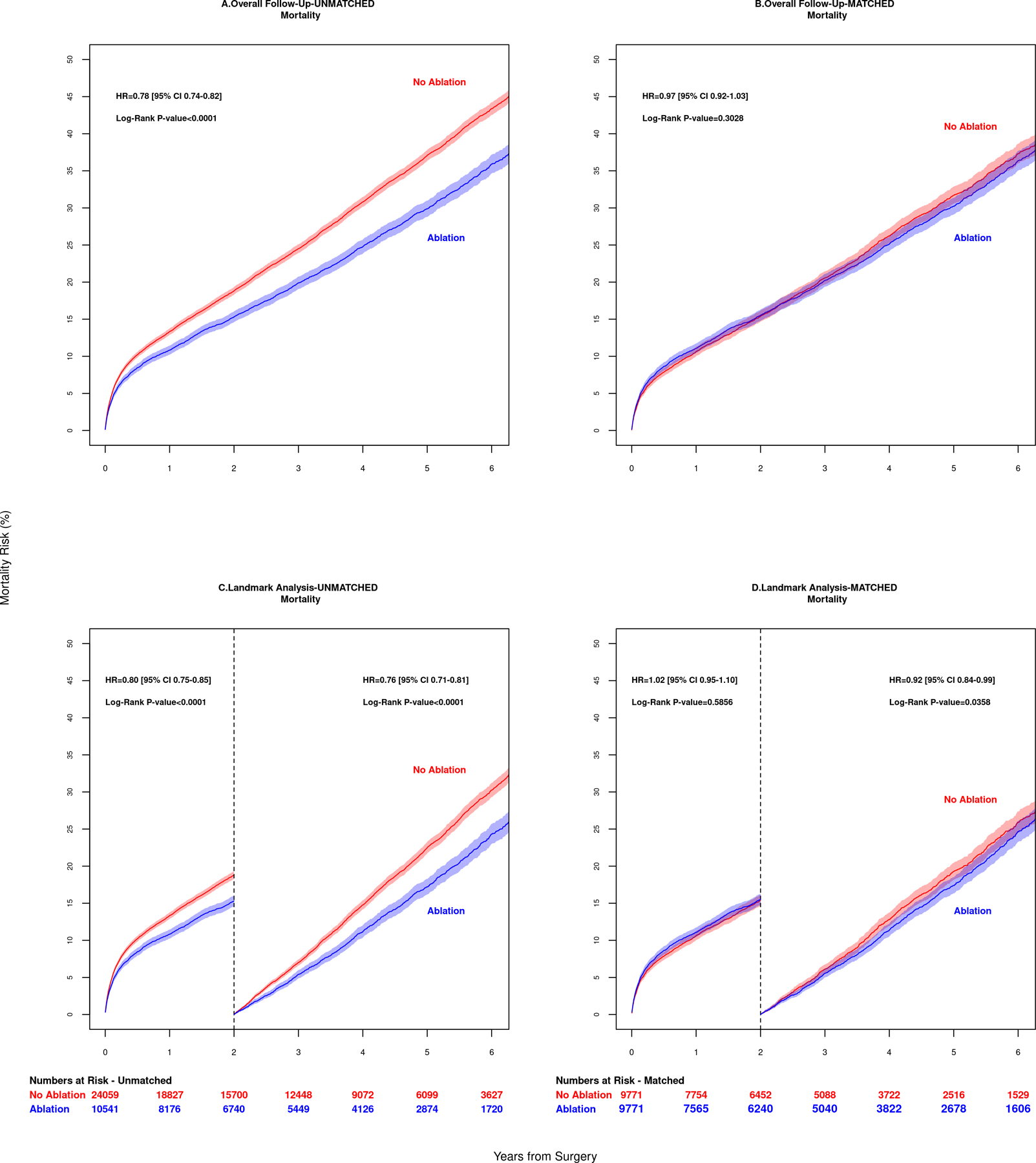
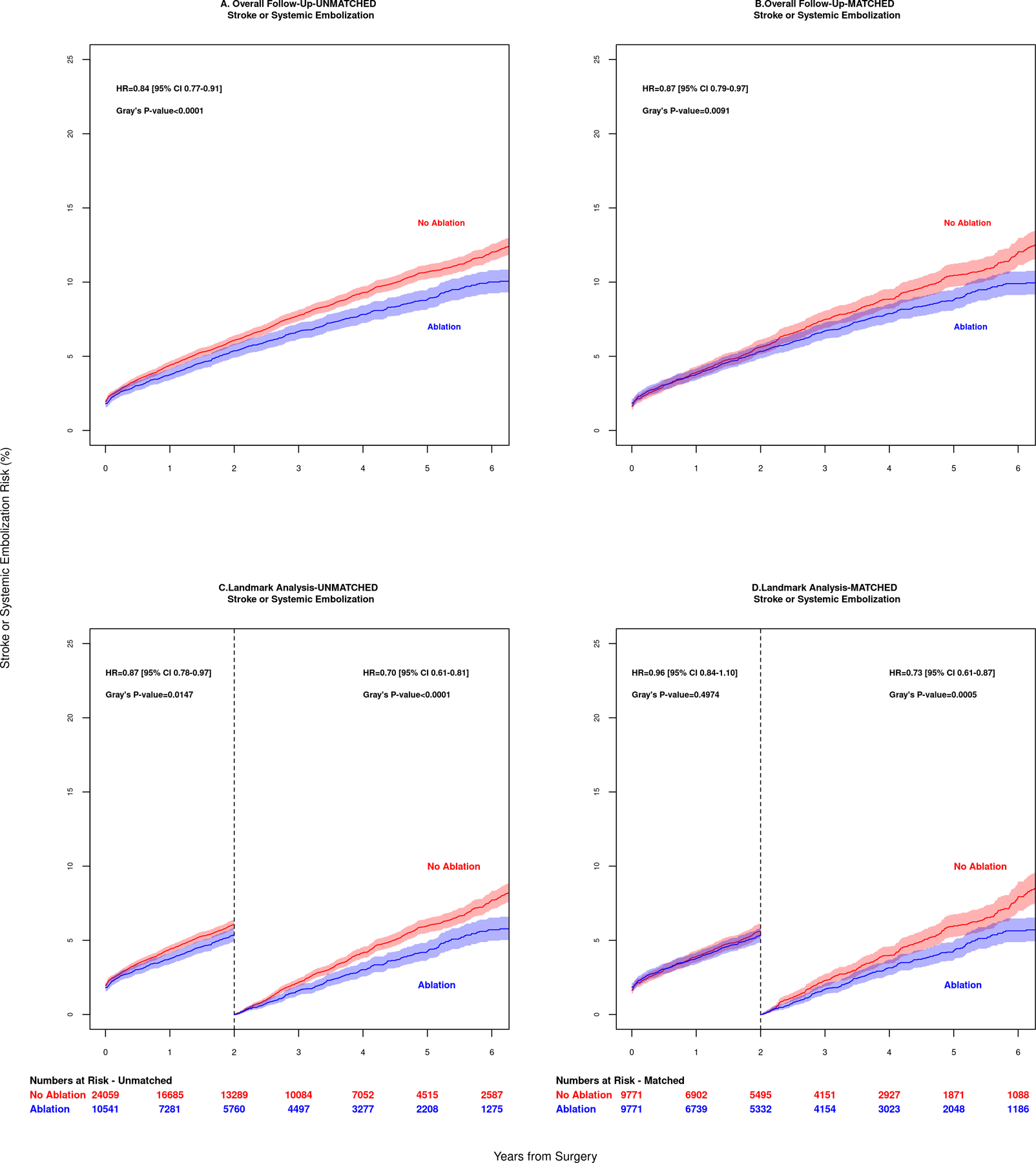
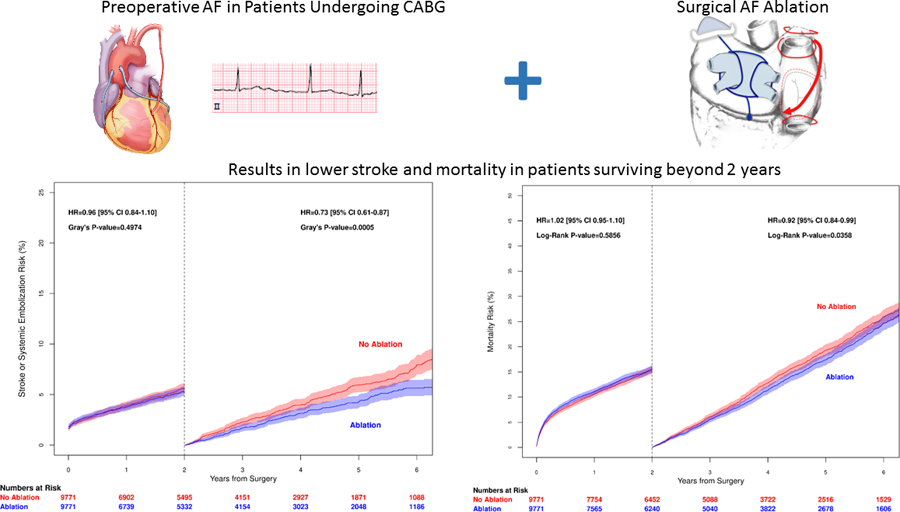
Results: Long-term mortality in propensity score-matched CABG patients (mean age 74 years; Society of Thoracic Surgeons risk score, 2.25) receiving ablation versus no ablation was similar (log-rank P = .30). Stroke or systemic embolization occurred in 2.2% versus 2.1% at 30 days and 9.9% versus 12.0% at 5 years (Gray P = .0091). Landmark analysis from 2 to 5 years showed lower mortality (hazard ratio, 0.89; 95% confidence interval 0.82-0.97; P = .0358) and lower risk of stroke or systemic embolization (hazard ratio, 0.73; 95% confidence interval, 0.61-0.87; P = .0006) in the ablation group.
Conclusions: Concomitant ablation in CABG patients with preoperative atrial fibrillation is associated with lower stroke or systemic embolization and mortality in patients who survive more than 2 years.
Keywords: ablation; atrial fibrillation; coronary artery bypass grafting; maze.
Copyright © 2019 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Commentary: Surgical ablation-Just do it!J Thorac Cardiovasc Surg. 2021 Apr;161(4):1262-1263. doi: 10.1016/j.jtcvs.2019.11.034. Epub 2019 Nov 27. J Thorac Cardiovasc Surg. 2021. PMID: 31859071 No abstract available.
-
Commentary: Questionable statistical routines.J Thorac Cardiovasc Surg. 2021 Apr;161(4):1263-1265. doi: 10.1016/j.jtcvs.2019.12.034. Epub 2020 Jan 3. J Thorac Cardiovasc Surg. 2021. PMID: 32005577 No abstract available.
References
-
- Malaisrie SC, McCarthy PM, Kruse J, Matsouaka R, Andrei AC, Grau-Sepulveda MV, et al. Burden of preoperative atrial fibrillation in patients undergoing coronary artery bypass grafting. The Journal of thoracic and cardiovascular surgery 2018. - PubMed
-
- Saxena A, Virk SA, Bowman S, Chan L, Jeremy R, Bannon PG. Preoperative atrial fibrillation portends poor outcomes after coronary bypass graft surgery: A systematic review and meta-analysis. The Journal of thoracic and cardiovascular surgery 2018;155:1524–1533 e1522. - PubMed
-
- Damiano RJ, Jr.,Gaynor SL, Bailey M, Prasad S, Cox JL, Boineau JP, et al. The long-term outcome of patients with coronary disease and atrial fibrillation undergoing the Cox maze procedure. The Journal of thoracic and cardiovascular surgery 2003;126:2016–2021. - PubMed
-
- Akpinar B, Sanisoglu I, Guden M, Sagbas E, Caynak B, Bayramoglu Z. Combined off-pump coronary artery bypass grafting surgery and ablative therapy for atrial fibrillation: early and mid-term results. The Annals of thoracic surgery 2006;81:1332–1337. - PubMed
-
- Geidel S, Lass M, Krause K, Schneider C, Boczor S, Kuck KH, et al. Persistent atrial fibrillation ablation concomitant to coronary surgery. Thorac Cardiovasc Surg 2011;59:207–212. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
