

Large-scale Analyses of Disease Biomarkers and Apremilast Pharmacodynamic Effects
- PMID: 31953524
- PMCID: PMC6969165
- DOI: 10.1038/s41598-020-57542-5
Large-scale Analyses of Disease Biomarkers and Apremilast Pharmacodynamic Effects
Abstract
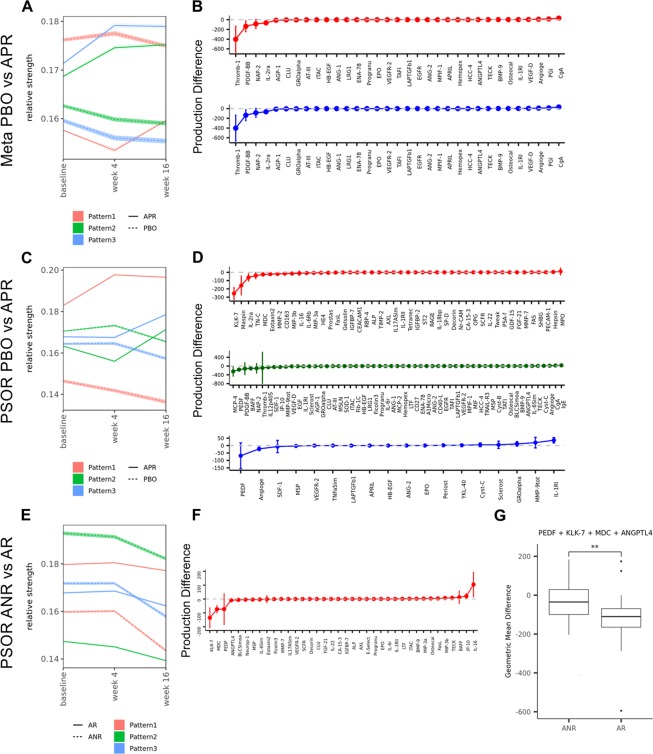
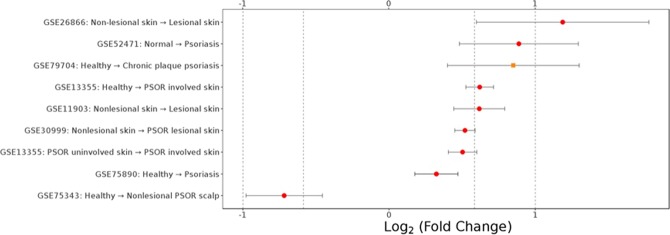
Finding biomarkers that provide shared link between disease severity, drug-induced pharmacodynamic effects and response status in human trials can provide number of values for patient benefits: elucidating current therapeutic mechanism-of-action, and, back-translating to fast-track development of next-generation therapeutics. Both opportunities are predicated on proactive generation of human molecular profiles that capture longitudinal trajectories before and after pharmacological intervention. Here, we present the largest plasma proteomic biomarker dataset available to-date and the corresponding analyses from placebo-controlled Phase III clinical trials of the phosphodiesterase type 4 inhibitor apremilast in psoriasis (PSOR), psoriatic arthritis (PsA), and ankylosing spondylitis (AS) from 526 subjects overall. Using approximately 150 plasma analytes tracked across three time points, we identified IL-17A and KLK-7 as biomarkers for disease severity and apremilast pharmacodynamic effect in psoriasis patients. Combined decline rate of KLK-7, PEDF, MDC and ANGPTL4 by Week 16 represented biomarkers for the responder subgroup, shedding insights into therapeutic mechanisms. In ankylosing spondylitis patients, IL-6 and LRG-1 were identified as biomarkers with concordance to disease severity. Apremilast-induced LRG-1 increase was consistent with the overall lack of efficacy in ankylosing spondylitis. Taken together, these findings expanded the mechanistic knowledge base of apremilast and provided translational foundations to accelerate future efforts including compound differentiation, combination, and repurposing.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
