

Complications in cranioplasty after decompressive craniectomy: timing of the intervention
- PMID: 31953606
- PMCID: PMC7184041
- DOI: 10.1007/s00415-020-09695-6
Complications in cranioplasty after decompressive craniectomy: timing of the intervention
Abstract
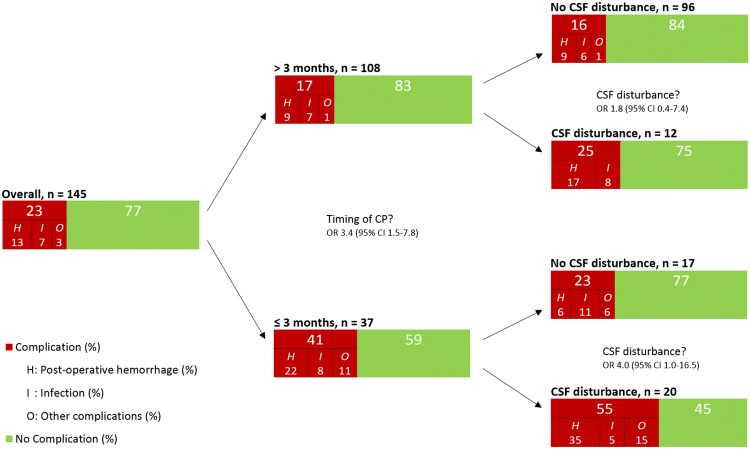
Objective: To prevent complications following decompressive craniectomy (DC), such as sinking skin flap syndrome, studies suggested early cranioplasty (CP). However, several groups reported higher complication rates in early CP. We studied the clinical characteristics associated with complications in patients undergoing CP, with special emphasis on timing.
Methods: A single-center observational cohort study was performed, including all patients undergoing CP from 2006 to 2018, to identify predictors of complications.
Results: 145 patients underwent CP: complications occurred in 33 (23%): 18 (12%) epi/subdural hemorrhage, 10 (7%) bone flap infection, 4 (3%) hygroma requiring drainage, and 1 (1%) post-CP hydrocephalus. On univariate analysis, acute subdural hematoma as etiology of DC, symptomatic cerebrospinal fluid (CSF) flow disturbance (hydrocephalus) prior to CP, and CP within three months after DC were associated with higher complication rates. On multivariate analysis, only acute subdural hematoma as etiology of DC (OR 7.5; 95% CI 1.9-29.5) and symptomatic CSF flow disturbance prior to CP (OR 2.9; 95% CI 1.1-7.9) were associated with higher complication rates. CP performed within three months after DC was not (OR 1.4; 95% CI 0.5-3.9). Pre-CP symptomatic CSF flow disturbance was the only variable associated with the occurrence of epi/subdural hemorrhage. (OR 3.8; 95% CI 1.6-9.0) CONCLUSION: Cranioplasty has high complication rates, 23% in our cohort. Contrary to recent systematic reviews, early CP was associated with more complications (41%), explained by the higher incidence of pre-CP CSF flow disturbance and acute subdural hematoma as etiology of DC. CP in such patients should therefore be performed with highest caution.
Keywords: Cranioplasty; Decompressive craniectomy; Hydrocephalus; Postoperative complications; Timing.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
