

Systemic therapy following craniotomy in patients with a solitary breast cancer brain metastasis
- PMID: 31953697
- PMCID: PMC7031200
- DOI: 10.1007/s10549-020-05531-7
Systemic therapy following craniotomy in patients with a solitary breast cancer brain metastasis
Abstract
Purpose: To describe practice patterns and patient outcomes with respect to the use of postoperative systemic therapy (ST) after resection of a solitary breast cancer brain metastasis (BCBM).
Methods: A multi-institutional retrospective review of consecutive patients undergoing resection of a single BCBM without extracranial metastases was performed to describe subtype-specific postoperative outcomes and assess the impact of types of ST on site of recurrence, progression-free survival (PFS), and overall survival (OS).
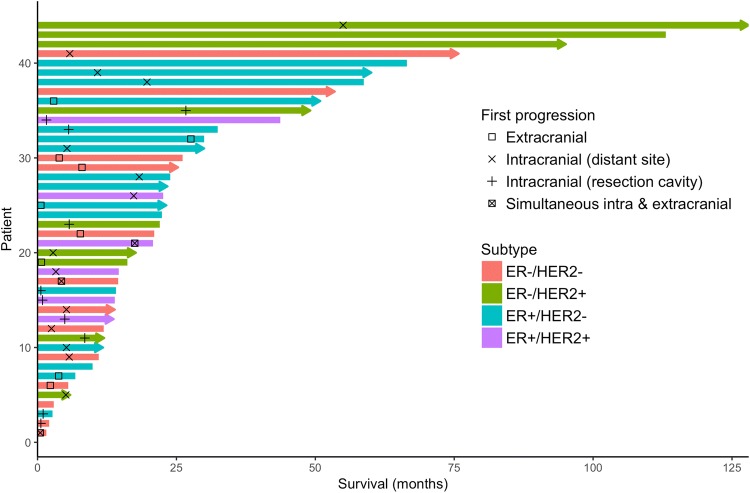
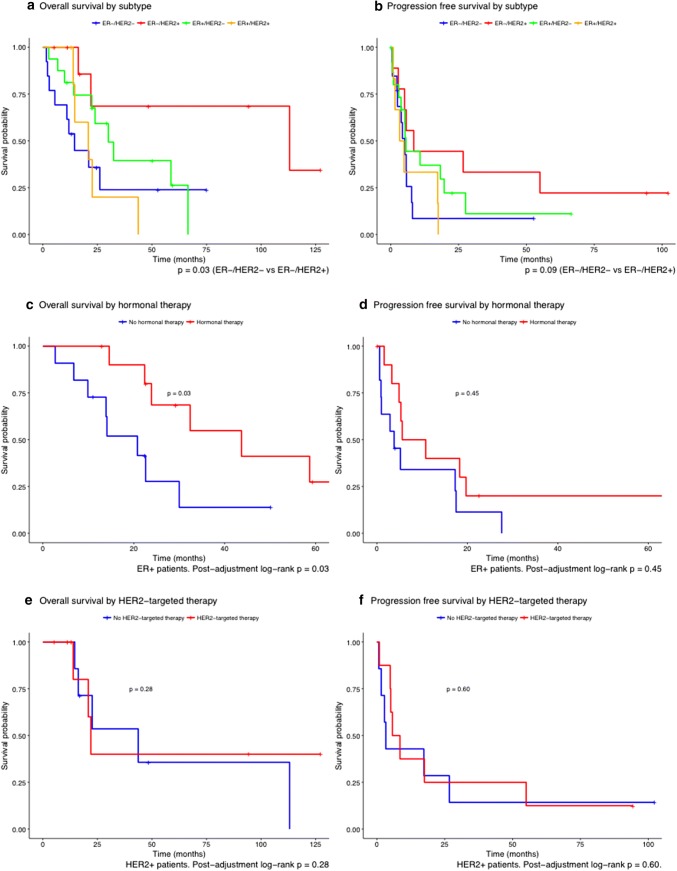
Results: Forty-four patients were identified. Stratified estimated survival was 15, 24, and 23 months for patients with triple negative, estrogen receptor positive (ER+), and HER2+ BCBMs, respectively. Patients receiving postoperative ST had a longer median PFS (8 versus 4 months, adjusted p-value 0.01) and OS (32 versus 15 months, adjusted p-value 0.21). Nine patients (20%) had extracranial progression, 23 (52%) had intracranial progression, three (8%) had both, and nine (20%) did not experience progression at last follow-up. Multivariate analysis showed that postoperative hormonal therapy was associated with longer OS (HR 0.26; 95% CI 0.08-0.89; p = 0.03) but not PFS (HR 0.35, 95% CI 0.08-1.47, p = 0.15) in ER+ patients. Postoperative HER2-targeted therapy was not associated with longer OS or PFS in HER2+ patients.
Conclusions: Disease progression occurred intracranially more often than extracranially following resection of a solitary BCBM. In ER+ patients, postoperative hormonal therapy was associated with longer OS. Postoperative HER2-targeted therapy did not show survival benefit in HER2+ patients. These results should be validated in larger cohorts.
Keywords: Breast cancer; Craniotomy; HER2-targeted therapy; Hormonal therapy; Solitary brain metastasis; Systemic therapy.
Conflict of interest statement
Priscilla K. Brastianos has received funding from Merck, BMS and Pfizer. She has received speaker’s Honoraria from Merck and Genentech-Roche and is a consultant for Tesaro, Angiochem, Genentech-Roche and Lilly. Nancy U. Lin has received funding for clinical trials from Genentech, Seattle Genetics, Novartis, Merck, and Pfizer, and has received compensation from Puma and Daiichi for service as a consultant. The other authors report no conflicts of interest.
Figures
References
-
- Boaziz C, Breau JL, Morere JF, Israel L. The blood–brain barrier: implications for chemotherapy in brain tumors. Pathol Biol. 1991;39(8):789–795. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
