

Liver function test abnormalities in a longitudinal cohort of Thai individuals treated since acute HIV infection
- PMID: 31953919
- PMCID: PMC6968973
- DOI: 10.1002/jia2.25444
Liver function test abnormalities in a longitudinal cohort of Thai individuals treated since acute HIV infection
Abstract
Introduction: Liver disease is a common cause of non-AIDS morbidity and mortality in people living with HIV (PLHIV), but the prevalence and significance of liver function test (LFT) abnormalities in early HIV infection is unknown. This study aimed to characterize LFTs in a large cohort of participants with acute HIV infection initiating immediate antiretroviral therapy (ART) and examine the association between LFTs and biomarkers of HIV infection and inflammation.
Methods: We measured LFTs at the time of HIV diagnosis and at 4, 12, 24 and 48 weeks after ART initiation in 426 Thai individuals with acute HIV infection from 2009 to 2018. A subset of individuals had data available at 96 and 144 weeks. We excluded individuals with concomitant viral hepatitis. Alanine aminotransferase (ALT) was the primary outcome of interest; values greater than 1.25 times the upper limit of normal were considered elevated. Analyses utilized descriptive statistics, non-parametric tests and multivariate logistic regression.
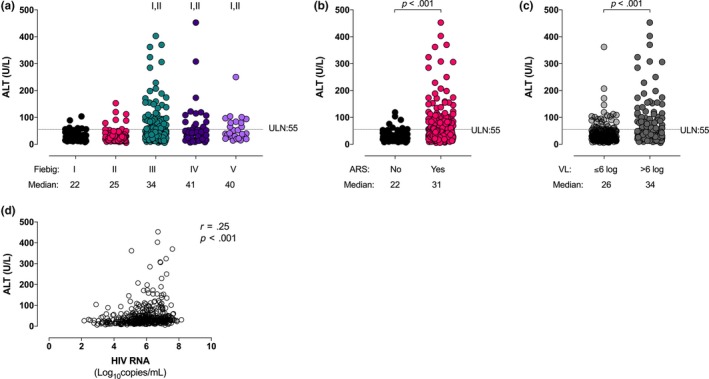
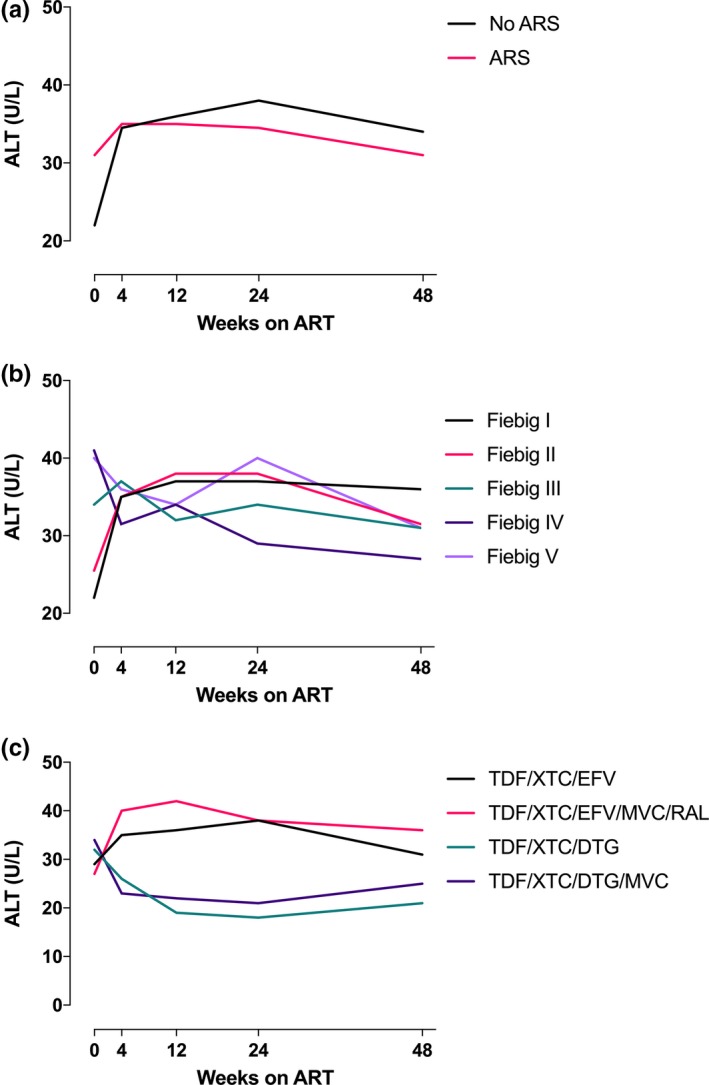
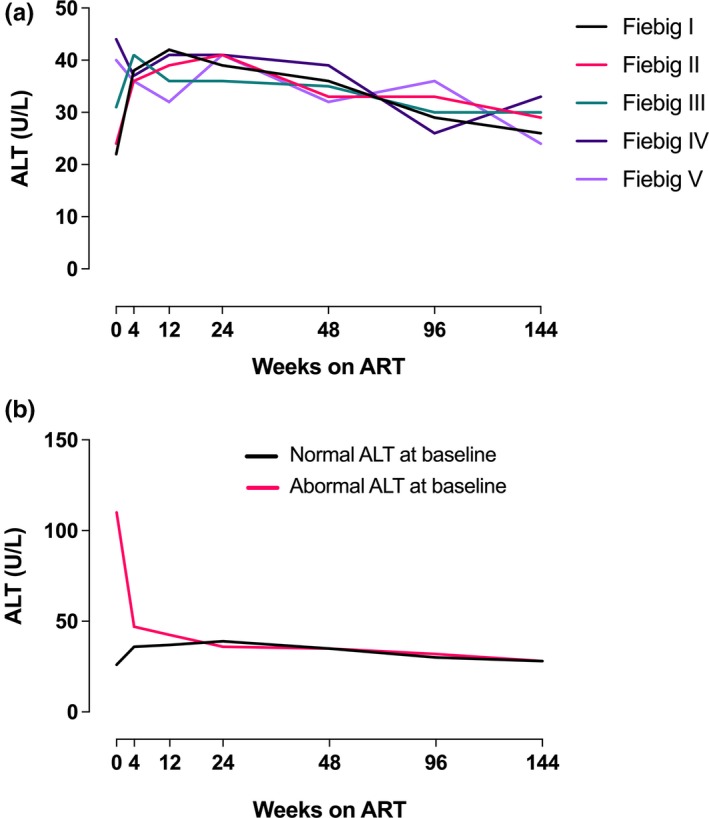
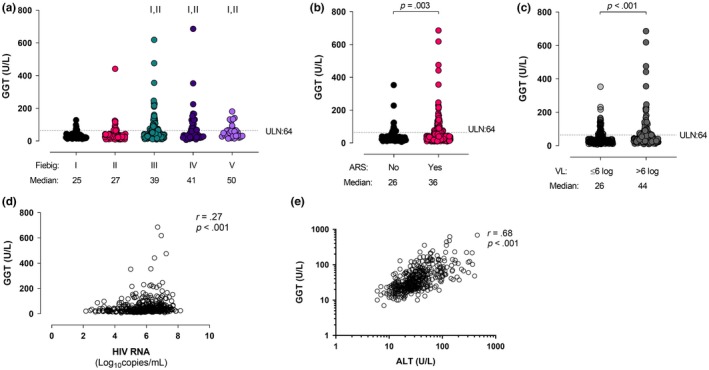
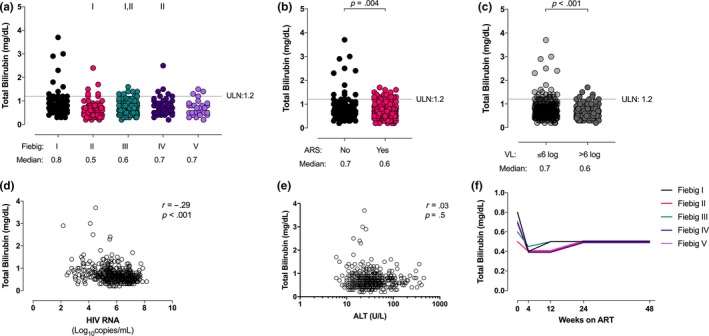
Results: Sixty-six of the 426 individuals (15.5%) had abnormal baseline ALT levels; the majority (43/66, 65.5%) had Grade 1 elevations. Elevated baseline ALT correlated with Fiebig stages III to V (p = 0.001) and baseline HIV RNA >6 log10 copies/mL (p = 0.012). Baseline elevations resolved by 48 weeks on ART in 59 of the 66 individuals (89%). ALT elevations at 24 and 48 weeks correlated with Fiebig stages I to II at diagnosis (p < 0.001), baseline plasma HIV RNA levels <6 log10 copies/mL (p < 0.001), abnormal baseline ALT (p < 0.001), baseline CD4 >350 cells/μL (p = 0.03) and older age (p = 0.03). Individuals initiating efavirenz-based regimens were more likely to have elevated ALT levels at 48 weeks compared with those on non-efavirenz-based regimens (p = 0.003).
Conclusions: One in six people with acute HIV infection have elevated LFTs. Clinical outcomes with ART started in acute HIV are generally good, with resolution of ALT elevations within 48 weeks on ART in most cases. These results suggest a multifactorial model for hepatic injury involving a combination of HIV-associated and ART-associated processes, which may change over time.
Keywords: Acquired Immunodeficiency Syndrome; HIV; Thailand; acute HIV; anti-HIV agents; antiretroviral agents; liver function tests.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- Rivero A, Mira JA, Pineda JA. Liver toxicity induced by non‐nucleoside reverse transcriptase inhibitors. J Antimicrob Chemother. 2007;59(3):342–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
