

Overcoming immunotherapeutic resistance by targeting the cancer inflammation cycle
- PMID: 31954172
- PMCID: PMC7363515
- DOI: 10.1016/j.semcancer.2020.01.002
Overcoming immunotherapeutic resistance by targeting the cancer inflammation cycle
Abstract
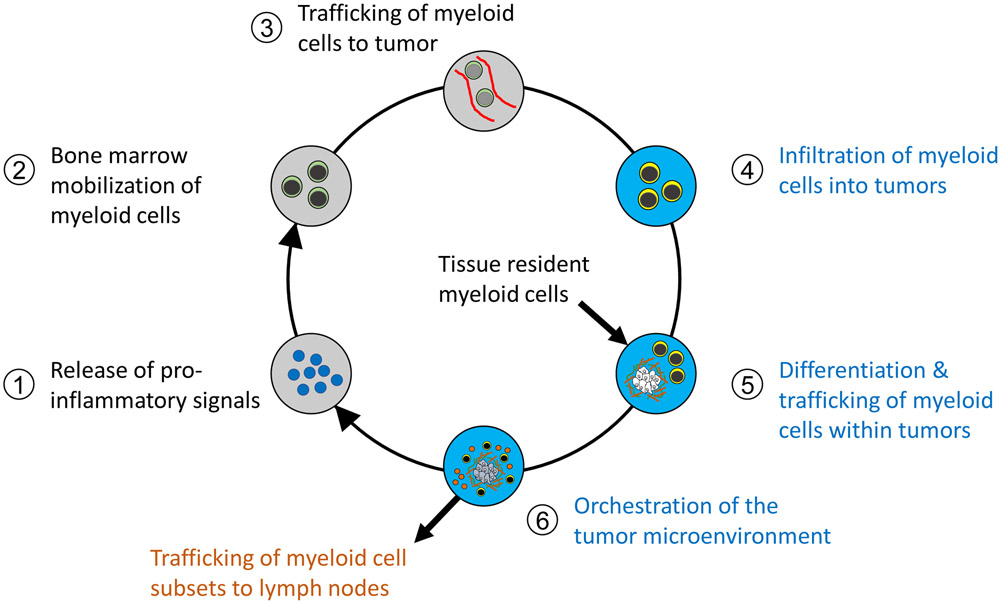
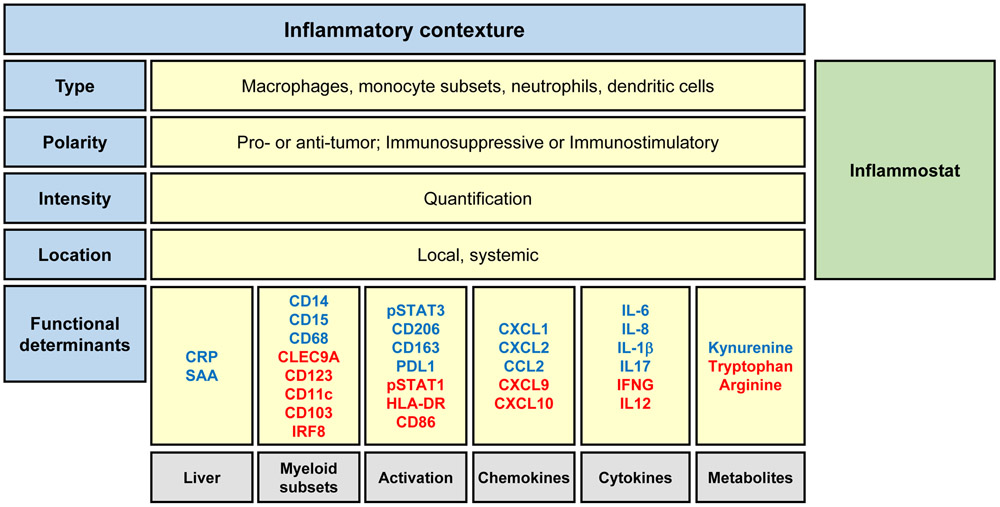
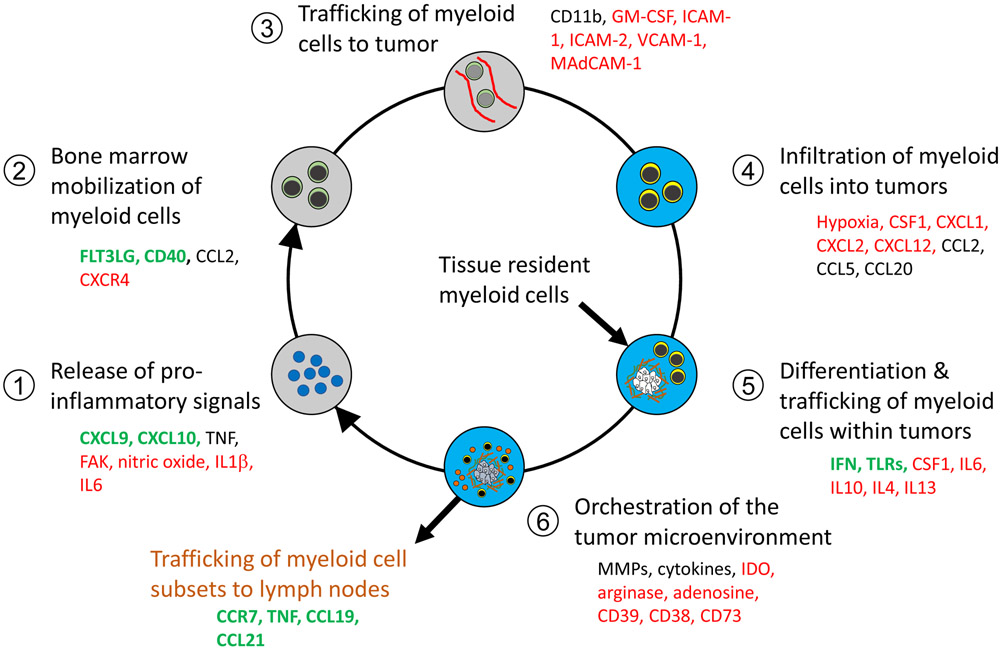
Inflammation is a hallmark of cancer and supports tumor growth, proliferation, and metastasis, but also inhibits T cell immunosurveillance and the efficacy of immunotherapy. The biology of cancer inflammation is defined by a cycle of distinct immunological steps that begins during disease conception with the release of inflammatory soluble factors. These factors communicate with host organs to trigger bone marrow mobilization of myeloid cells, trafficking of myeloid cells to the tumor, and differentiation of myeloid cells within the tumor bed. Tumor-infiltrating myeloid cells then orchestrate an immunosuppressive microenvironment and assist in sustaining a vicious cycle of inflammation that co-evolves with tumor cells. This Cancer-Inflammation Cycle acts as a rheostat or "inflammostat" that impinges upon T cell immunosurveillance and prevents the development of productive anti-tumor immunity. Here, we define the major nodes of the Cancer-Inflammation Cycle and describe their impact on T cell immunosurveillance in cancer. Additionally, we discuss emerging pre-clinical and clinical data suggesting that intervening upon the Cancer-Inflammation Cycle will be a necessary step for broadening the potential of immunotherapy in cancer.
Keywords: Cancer; Immunotherapy; Inflammation; Inflammostat; Macrophage; Myeloid cells; T cells.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest G.L.B. is a consultant/advisory board member for Seattle Genetics, Aduro Biotech, AstraZeneca, Bristol-Myers Squibb, Genmab, Merck, Shattuck Labs, Boehringer Ingelheim, and BiolineRx; reports receiving commercial research grants from Incyte, Bristol-Myers Squibb, Verastem, Halozyme, Biothera, Newlink, Novartis, and Janssen. G.L.B. is an inventor of intellectual property and recipient of royalties related to CAR T cells that are licensed by the University of Pennsylvania to Novartis. No additional potential conflicts of interest were disclosed by M.M.W.
Figures
References
-
- Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, Rodriguez-Abreu D, Moro-Sibilot D, Thomas CA, Barlesi F, Finley G, Kelsch C, Lee A, Coleman S, Deng Y, Shen Y, Kowanetz M, Lopez-Chavez A, Sandler A, Reck M, Group IMS, Atezolizumab for First-Line Treatment of Metastatic Nonsquamous NSCLC, N Engl J Med 378(24) (2018) 2288–2301. - PubMed
-
- Antonia SJ, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M, Cho BC, Bourhaba M, Quantin X, Tokito T, Mekhail T, Planchard D, Kim YC, Karapetis CS, Hiret S, Ostoros G, Kubota K, Gray JE, Paz-Ares L, de Castro Carpeno J, Wadsworth C, Melillo G, Jiang H, Huang Y, Dennis PA, Ozguroglu M, Durvalumab after Chemoradiotherapy in Stage III Non-Small-Cell Lung Cancer, N Engl J Med 377(20) (2017) 1919–1929. - PubMed
-
- Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O'Brien M, Rao S, Hotta K, Leiby MA, Lubiniecki GM, Shentu Y, Rangwala R, Brahmer JR, K.-. Investigators, Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer, N Engl J Med 375(19) (2016)1823–1833. - PubMed
-
- Borghaei H, Paz-Ares L, Horn L, Spigel DR, Steins M, Ready NE, Chow LQ, Vokes EE, Felip E, Holgado E, Barlesi F, Kohlhaufl M, Arrieta O, Burgio MA, Fayette J, Lena H, Poddubskaya E, Gerber DE, Gettinger SN, Rudin CM, Rizvi N, Crino L, Blumenschein GR Jr., Antonia SJ, Dorange C, Harbison CT, Graf Finckenstein F, Brahmer JR, Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer, N Engl J Med 373(17) (2015) 1627–39. - PMC - PubMed
-
- Motzer RJ, Tannir NM, McDermott DF, Aren Frontera O, Melichar B, Choueiri TK, Plimack ER, Barthelemy P, Porta C, George S, Powles T, Donskov F, Neiman V, Kollmannsberger CK, Salman P, Gurney H, Hawkins R, Ravaud A, Grimm MO, Bracarda S, Barrios CH, Tomita Y, Castellano D, Rini BI, Chen AC, Mekan S, McHenry MB, Wind-Rotolo M, Doan J, Sharma P, Hammers HJ, Escudier B, CheckMate I, Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma, N Engl J Med 378(14) (2018) 1277–1290. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
