

Comparing Risk Scores in the Prediction of Coronary and Cardiovascular Deaths: Coronary Artery Calcium Consortium
- PMID: 31954640
- PMCID: PMC7343587
- DOI: 10.1016/j.jcmg.2019.12.010
Comparing Risk Scores in the Prediction of Coronary and Cardiovascular Deaths: Coronary Artery Calcium Consortium
Abstract
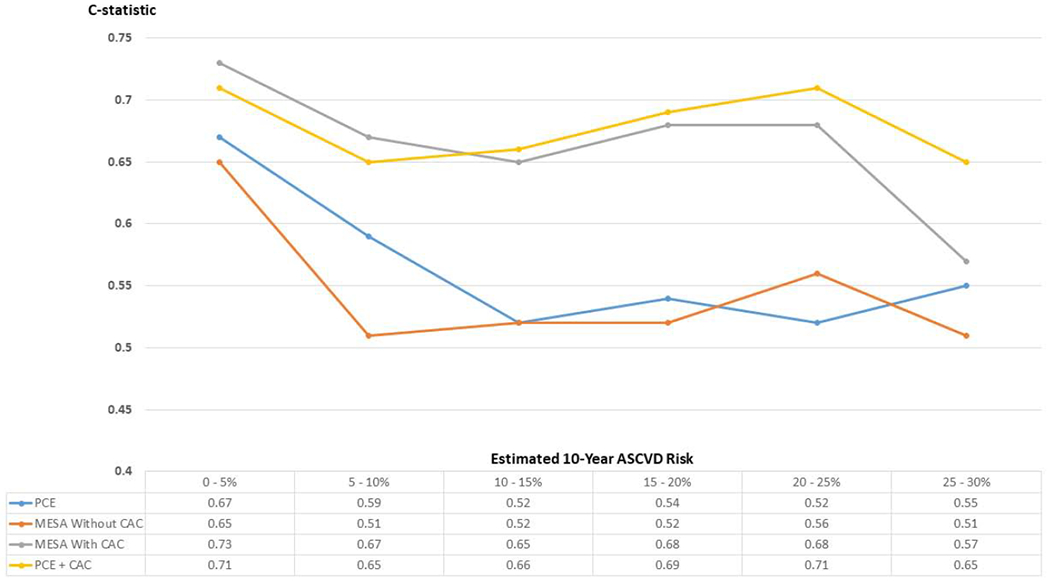
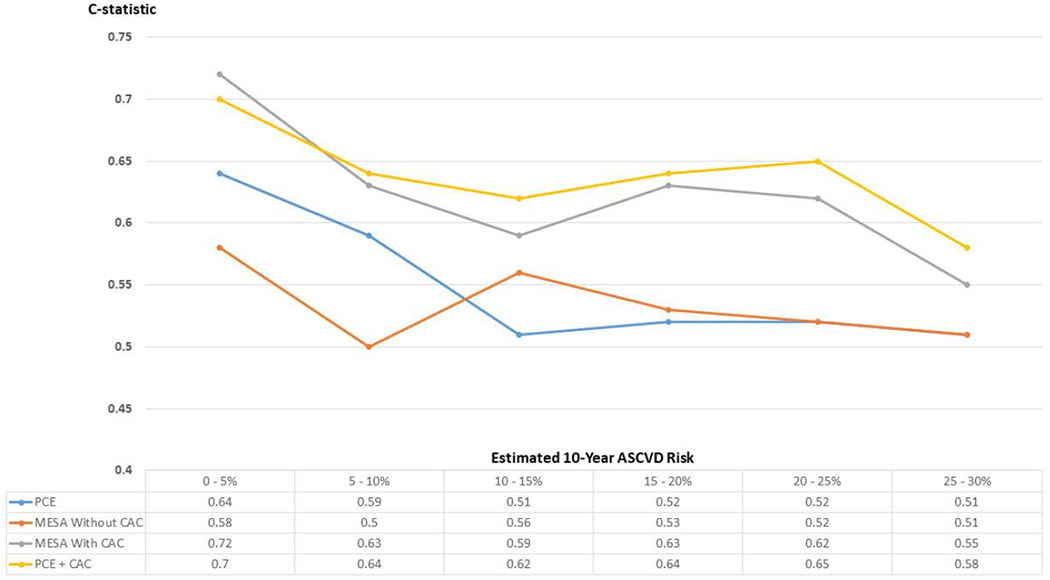
Objectives: This study compared risk discrimination for the prediction of coronary heart disease (CHD) and cardiovascular disease (CVD) deaths for the Pooled Cohort Equations (PCE), the MESA (Multi-Ethnic Study of Atherosclerosis) Risk Score (with and without coronary artery calcium [CAC]), and of simple addition of CAC to the PCE.
Background: The PCE predict 10-year risk of atherosclerotic CVD events, and the MESA Risk Score predicts risk of CHD. Their comparative performance for the prediction of fatal events is poorly understood.
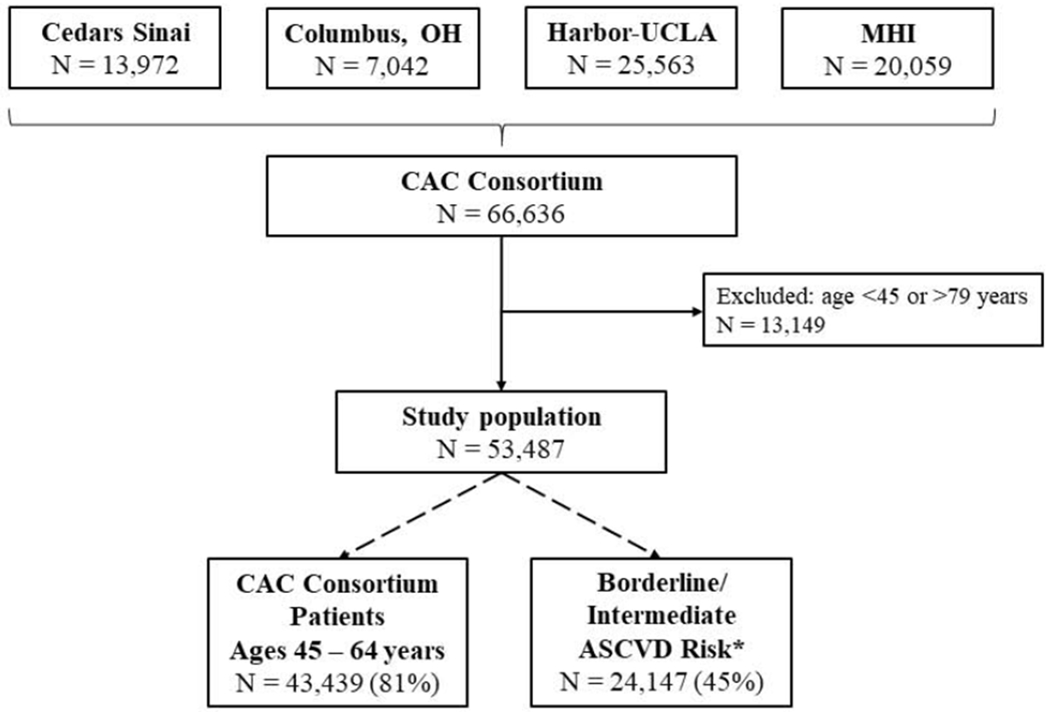
Methods: We evaluated 53,487 patients ages 45 to 79 years from the CAC Consortium, a retrospective cohort study of asymptomatic individuals referred for clinical CAC scoring. Risk discrimination was measured using C-statistics.
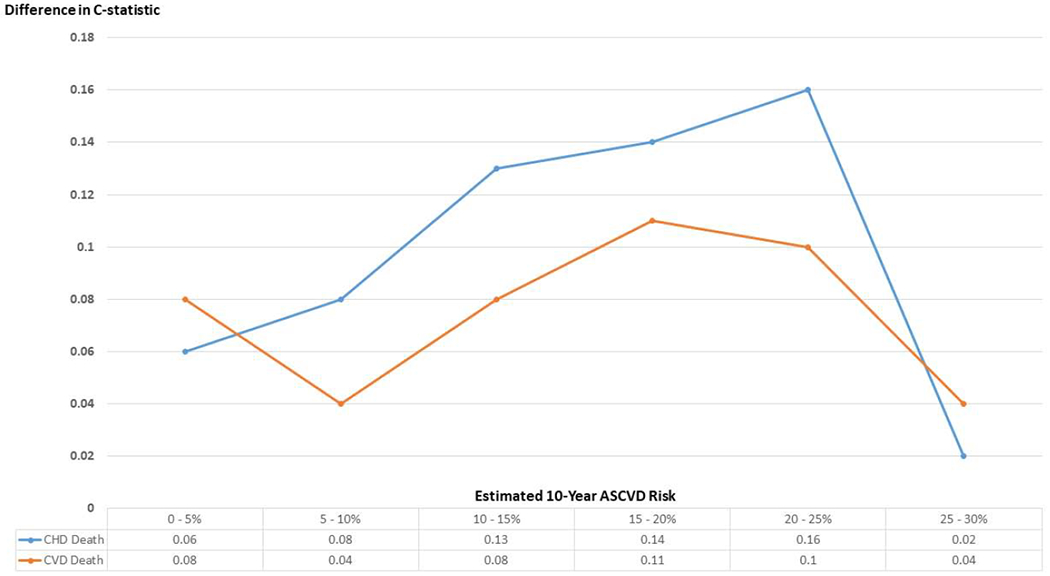
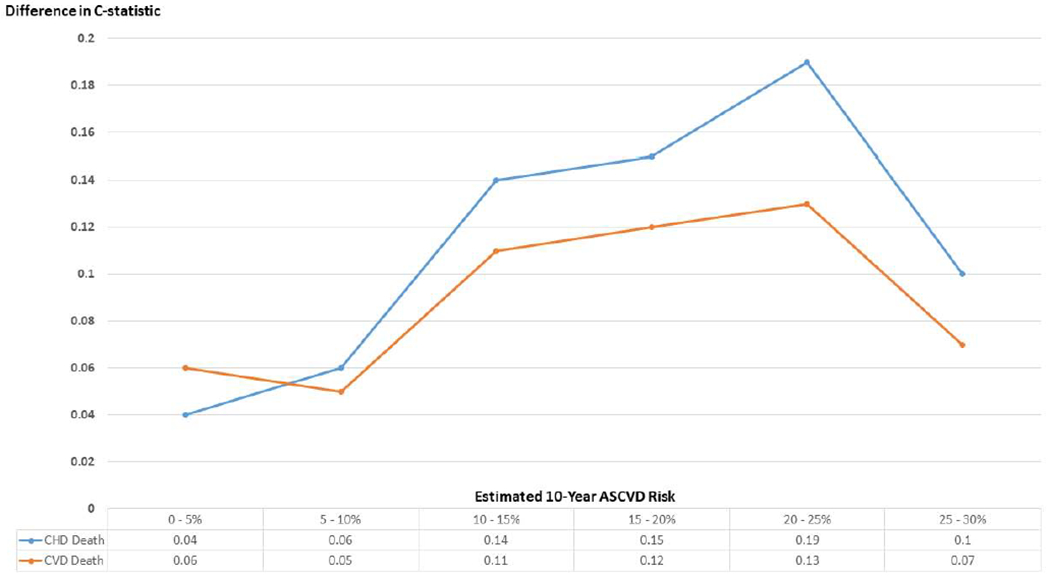
Results: Mean age was 57 years, 35% were women, and 39% had CAC of 0. There were 421 CHD and 775 CVD deaths over a mean 12-year follow-up. In the overall study population, discrimination with the MESA Risk Score with CAC and the PCE was almost identical for both outcomes (C-statistics: 0.80 and 0.79 for CHD death, 0.77 and 0.78 for CVD death, respectively). Addition of CAC to the PCE improved risk discrimination, yielding the largest C-statistics. The MESA Risk Score with CAC and the PCE plus CAC showed the best discrimination among the 45% of patients with 5% to 20% estimated risk. Secondary analyses by estimated CVD risk strata showed modestly improved risk discrimination with CAC also among low- and high-estimated risk groups.
Conclusions: Our findings support the current guideline recommendation to use, among available risk scores, the PCE for initial risk assessment and to use CAC for further risk assessment in a broad borderline and intermediate risk group. Also, in select individuals at low or high estimated risk, CAC modestly improved discrimination. Studies in unselected populations will lead to further understanding of the potential value of tools combining risk scores and CAC for optimal risk assessment.
Keywords: cardiovascular disease; coronary artery calcium; mortality; risk; score.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr. Blaha was supported by National Institutes of Health award L30 HL110027 for this project. Dr. Budoff has received grant support from General Electric. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Incorporating Coronary Calcium Scoring Into Risk Assessment For Primary Prevention.JACC Cardiovasc Imaging. 2021 Feb;14(2):422-425. doi: 10.1016/j.jcmg.2020.12.012. JACC Cardiovasc Imaging. 2021. PMID: 33541530 No abstract available.
References
-
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139:e1082–e1143. - PMC - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J. 2016;37:2315–2381. - PMC - PubMed
-
- Anderson TJ, Grégoire J, Pearson GJ, et al. 2016 Canadian Cardiovascular Society Guidelines for the Management of Dyslipidemia for the Prevention of Cardiovascular Disease in the Adult. Can J Cardiol. 2016;32:1263–1282. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2018;138(17):e484–e594. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
