

Prevalence of steatosis and fibrosis in young adults in the UK: a population-based study
- PMID: 31954687
- PMCID: PMC7026693
- DOI: 10.1016/S2468-1253(19)30419-4
Prevalence of steatosis and fibrosis in young adults in the UK: a population-based study
Abstract
Background: The estimated worldwide prevalence of non-alcoholic fatty liver disease (NAFLD) in adults is 25%; however, prevalence in young adults remains unclear. We aimed to identify the prevalence of steatosis and fibrosis in young adults in a sample of participants recruited through the Avon Longitudinal Study of Parents and Children (ALSPAC), based on transient elastography and controlled attenuation parameter (CAP) score.
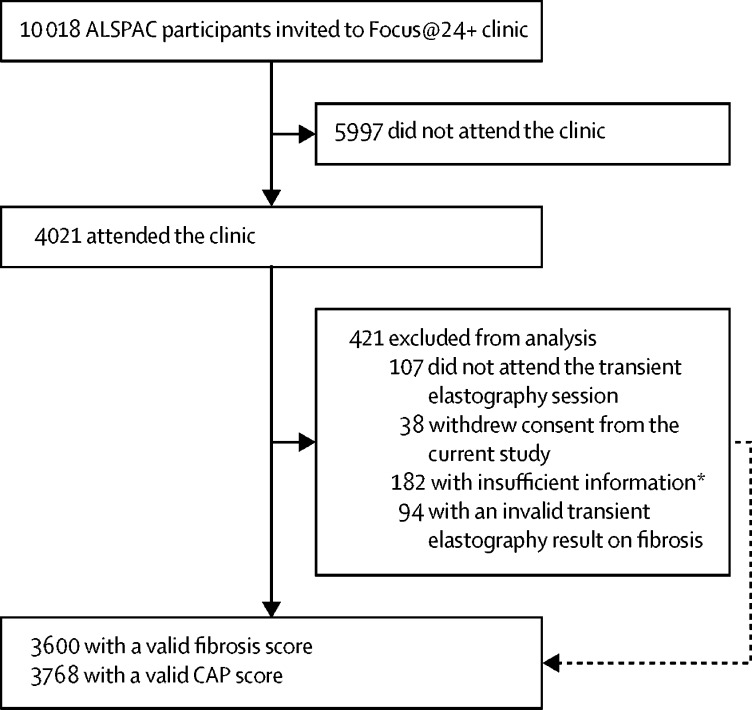
Methods: In this population-based study, we invited active participants of the ALSPAC cohort to our Focus@24+ clinic at the University of Bristol (Bristol, UK) between June 5, 2015, and Oct 31, 2017, for assessment by transient elastography with FibroScan, to determine the prevalence of steatosis and fibrosis. FibroScan data were collected on histologically equivalent fibrosis stage (F0-F4) and steatosis grade (S0-S3); results with an IQR to median ratio of 30% or greater were excluded for median fibrosis results greater than 7·1 kPa, and CAP scores for steatosis were excluded if less than ten valid readings could be obtained. Results were collated with data on serology (including alanine aminotransferase, aspartate aminotransferase, and γ-glutamyl transferase) and exposures of interest: alcohol consumption (via the Alcohol Use Disorder Identification Test for Consumption [AUDIT-C] and the Diagnostic and Statistical Manual of Mental Disorders-5 criteria for alcohol use disorder), body-mass index (BMI), waist-to-height ratio, socioeconomic status (based on predefined ALSPAC markers), and sex. We used logistic regression models to calculate odds ratios (ORs) for the effect of exposures of interest on risk of steatosis and fibrosis, after dichotomising the prevalences of fibrosis and steatosis and adjusting for covariates (excessive alcohol intake [hazardous drinking, AUDIT-C score ≥5; or harmful drinking, evidence of alcohol use disorder], social class, smoking, and BMI).
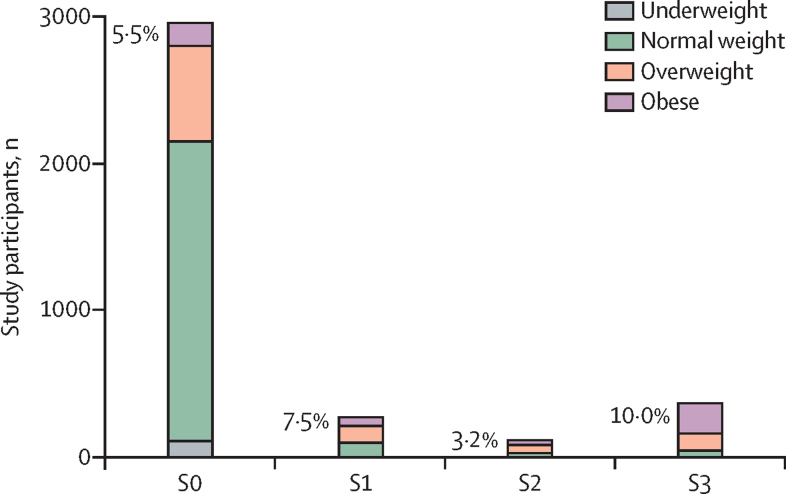
Findings: 10 018 active ALSPAC participants were invited to our Focus@24+ clinic, and 4021 attended (1507 men and 2514 women), with a mean age of 24·0 years (IQR 23·0-25·0). 3768 CAP scores were eligible for analysis. 780 (20·7% [95% CI 19·4-22·0]) participants had suspected steatosis (S1-S3; ≥248 dB/m), with 377 (10·0%) presenting with S3 (severe) steatosis (≥280 dB/m). A BMI in the overweight or obese range was positively associated with steatosis when adjusted for excessive alcohol consumption, social class, and smoking (overweight BMI: OR 5·17 [95% CI 4·11-6·50], p<0·0001; obese BMI: 27·27 [20·54-36·19], p<0·0001). 3600 participants had valid transient elastography results for fibrosis analysis. 96 participants (2·7% [95% CI 2·2-3·2]) had transient elastography values equivalent to suspected fibrosis (F2-F4; ≥7·9 kPa), nine of whom had values equivalent to F4 fibrosis (≥11·7 kPa). Individuals with alcohol use disorder and steatosis had an increased risk of fibrosis when adjusted for smoking and social class (4·02 [1·24-13·02]; p=0·02).
Interpretation: One in five young people had steatosis and one in 40 had fibrosis around the age of 24 years. The risk of fibrosis appears to be greatest in young adults who have harmful drinking patterns and steatosis. A holistic approach to the UK obesity epidemic and excessive drinking patterns is required to prevent an increasing health-care burden of adults with advanced liver disease in later life.
Funding: Medical Research Council UK, Alcohol Change UK, David Telling Charitable Trust.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Fatty liver disease: putting the spotlight on a silent menace for young adults.Lancet Gastroenterol Hepatol. 2020 Mar;5(3):236-238. doi: 10.1016/S2468-1253(19)30420-0. Epub 2020 Jan 15. Lancet Gastroenterol Hepatol. 2020. PMID: 31954686 No abstract available.
References
-
- Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther. 2011;34:274–285. - PubMed
-
- Margini C, Dufour JF. The story of HCC in NAFLD: from epidemiology, across pathogenesis, to prevention and treatment. Liver Int. 2016;36:317–324. - PubMed
-
- Williams R, Alexander G, Armstrong I. Disease burden and costs from excess alcohol consumption, obesity, and viral hepatitis: fourth report of the Lancet Standing Commission on Liver Disease in the UK. Lancet. 2018;391:1097–1107. - PubMed
-
- de Graaf EL, Kench J, Dilworth P. Grade of deceased donor liver macrovesicular steatosis impacts graft and recipient outcomes more than the donor risk index. J Gastroenterol Hepatol. 2012;27:540–546. - PubMed
-
- Doycheva I, Watt KD, Alkhouri N. Nonalcoholic fatty liver disease in adolescents and young adults: the next frontier in the epidemic. Hepatology. 2017;65:2100–2109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
