

Utilization and Outcomes of Surgical Castration in Comparison to Medical Castration in Metastatic Prostate Cancer
- PMID: 31956009
- PMCID: PMC7190190
- DOI: 10.1016/j.clgc.2019.09.020
Utilization and Outcomes of Surgical Castration in Comparison to Medical Castration in Metastatic Prostate Cancer
Abstract
Background: Androgen deprivation therapy (ADT) is the gold standard for metastatic prostate cancer, which can be achieved either by surgical or medical castration. In this study, we evaluated the trends of utilization of surgical castration and also assess the survival differences of patients who underwent surgical castration when compared with those who underwent medical castration.
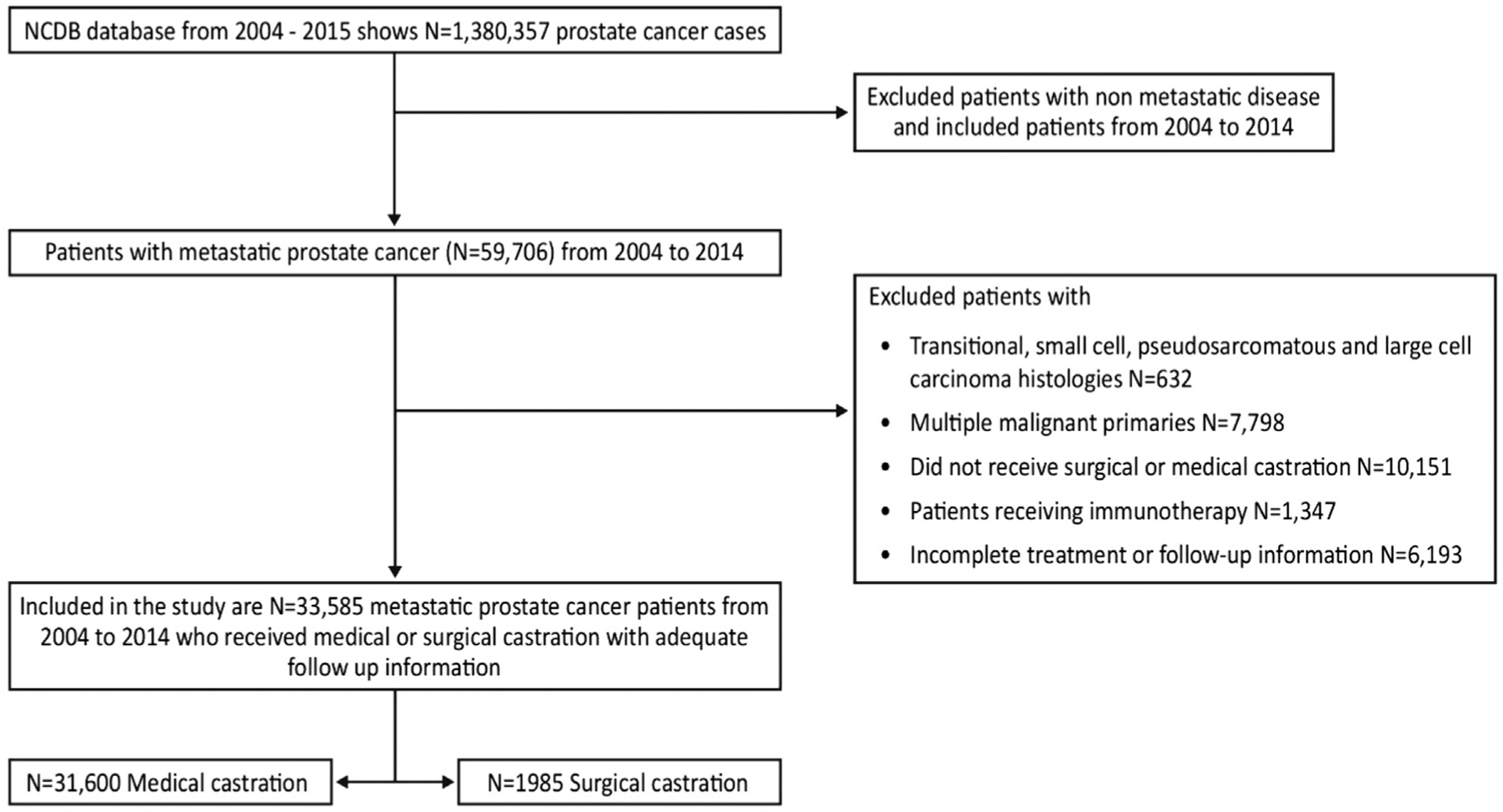
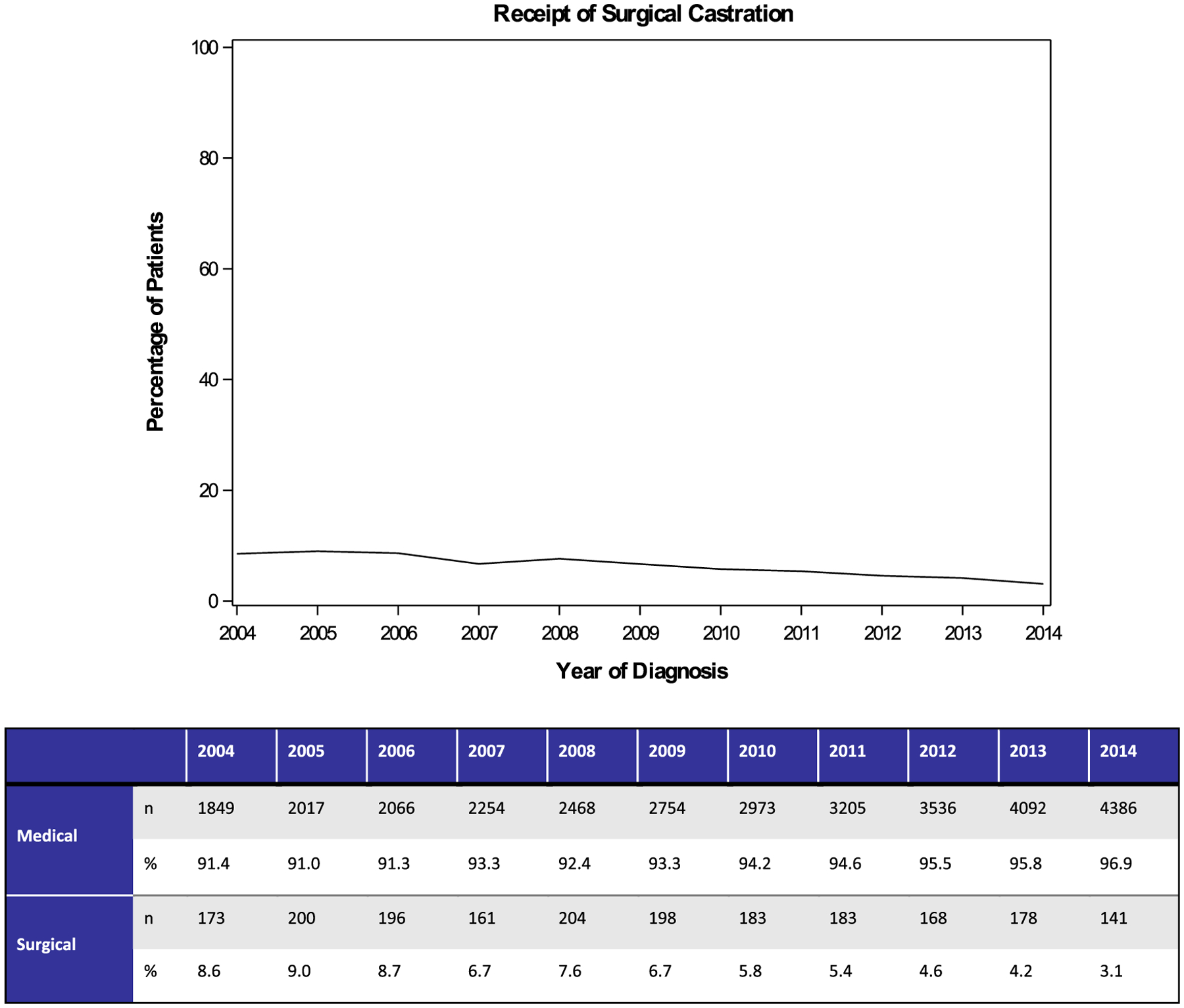
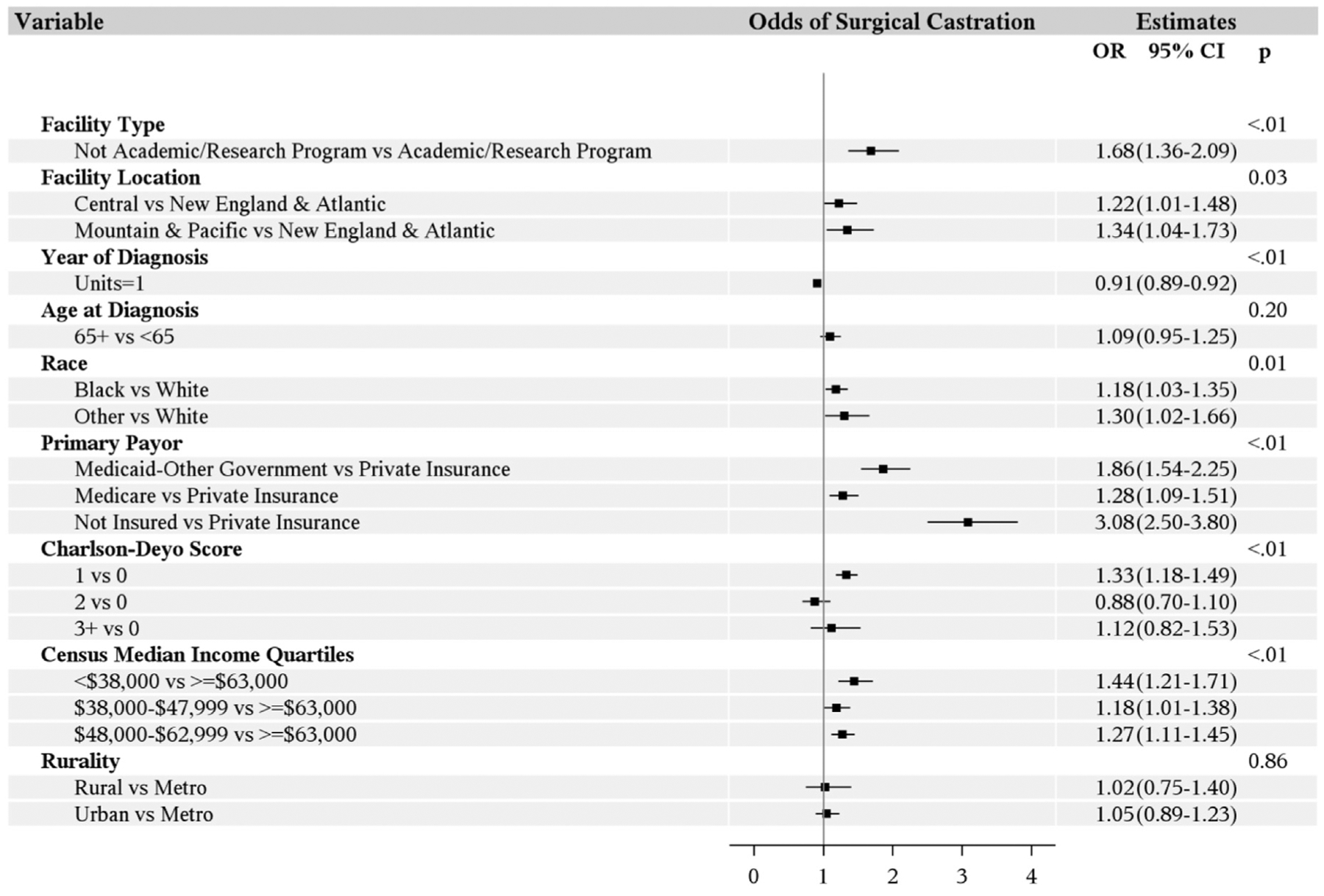
Materials and methods: The National Cancer Database was used to identify patients with metastatic prostate cancer from 2004 to 2014. Cochran-Armitage tests were used to assess temporal trends in the proportion of patients receiving surgical castration relative to medical castration. Logistic and Cox regression models were utilized to estimate the odds of utilization of surgical castration and the effect of castration on overall survival (OS).
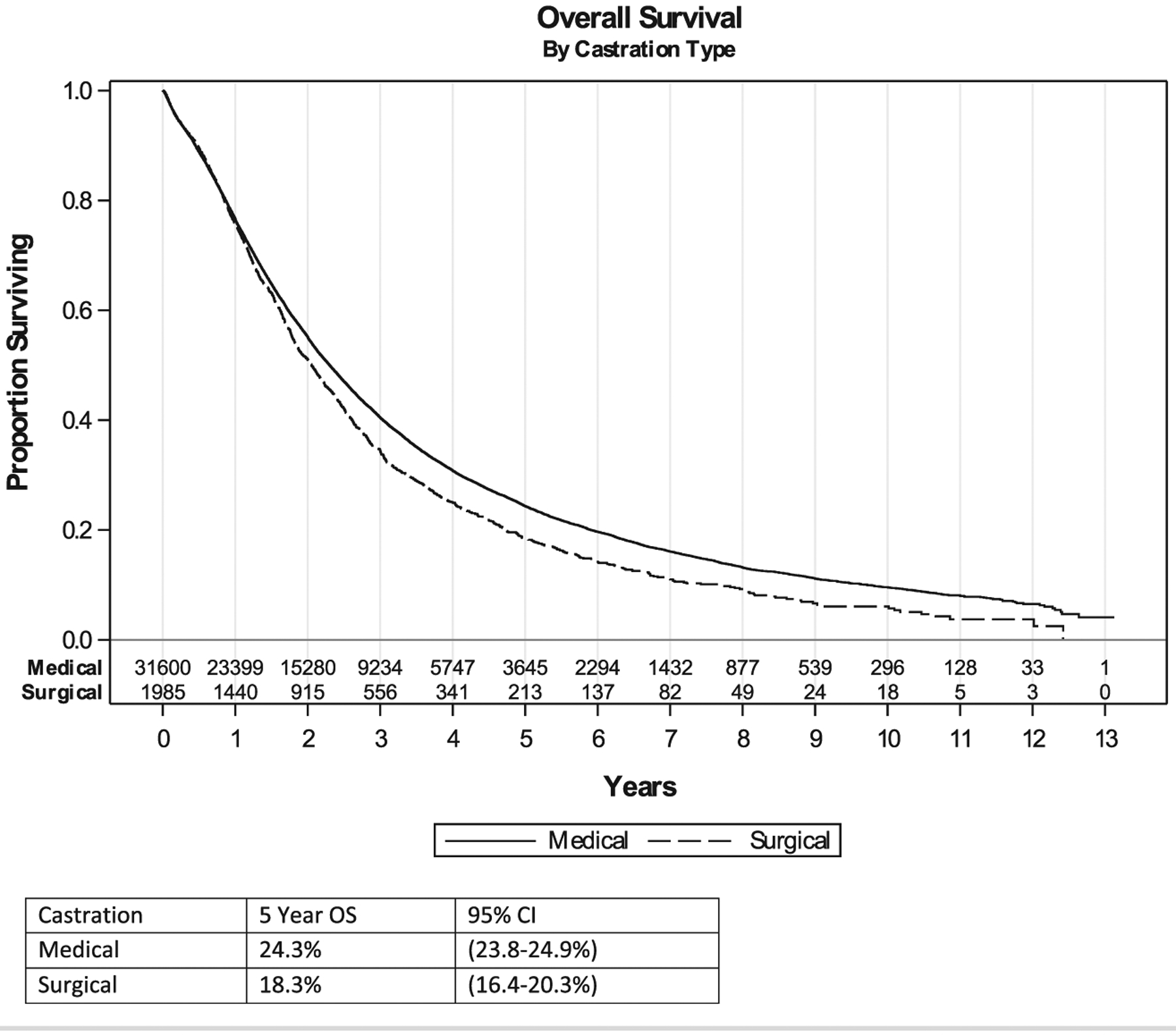
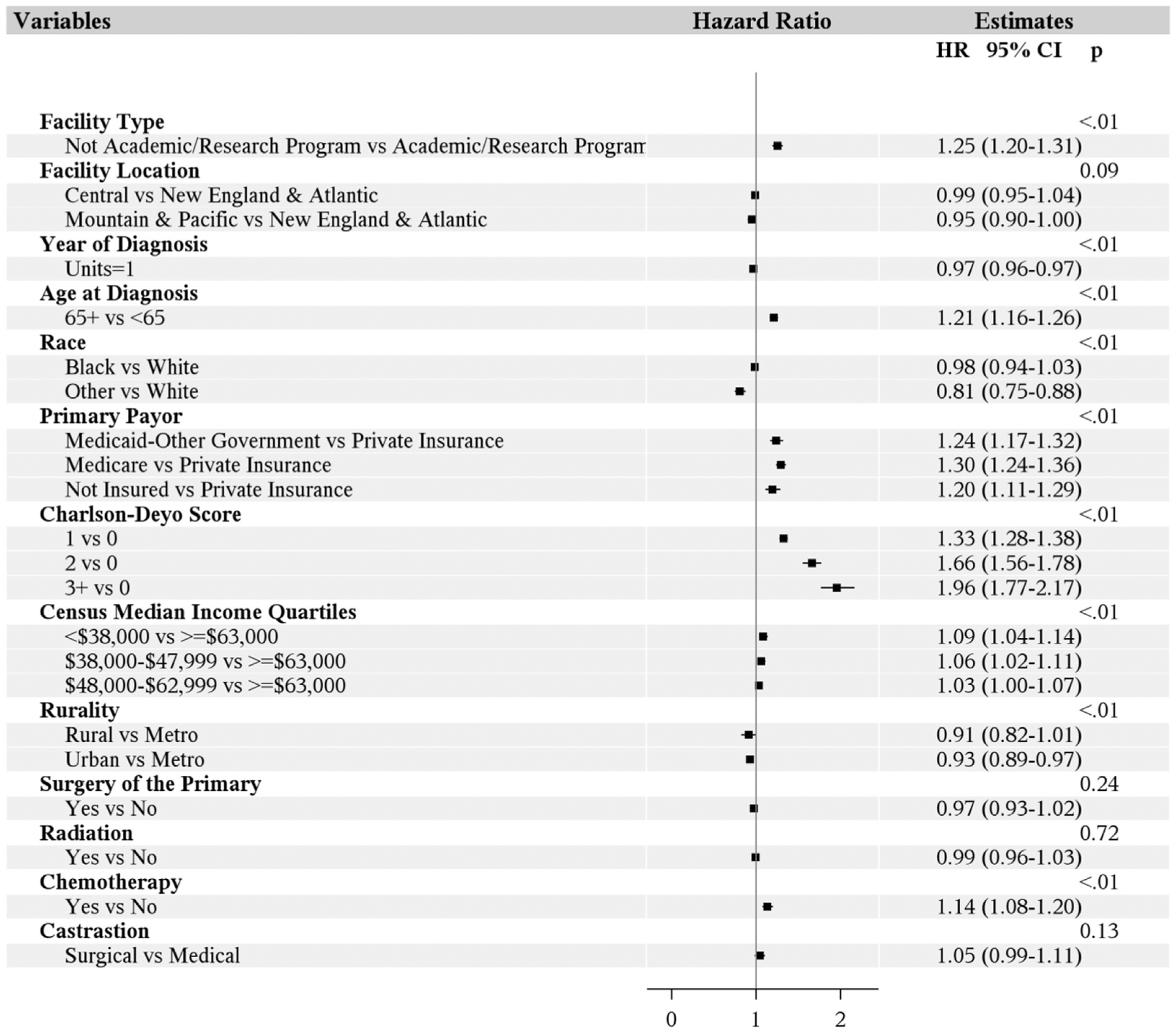
Results: A total of 33,585 patients with metastatic prostate cancer were identified; 31,600 (94.1%) had medical castration, and 1985 (5.9%) underwent surgical castration. There was significant decline in the trend of utilization of surgical castration from 8.6% in 2004 to 3.1% in 2014. On multivariable analysis, being of a non-Caucasian race, having lower median income levels, having non-private insurance, and earlier years of diagnosis were found to be associated with increased odds of choosing surgical castration over medical castration. Notably, the odds of surgical castration were lower at academic centers. On univariable analysis, a survival difference between castration modality was evidenced (P < .01); 5-year OS for medical castration and surgical castration were 24.3% and 18.2%, respectively. However, on multivariable analysis, there was no OS difference between surgical castration and medical castration (P = .13).
Conclusions: In this large contemporary analysis, the utilization of surgical castration has declined over time, with no OS difference when compared with medical castration. Increasing the utilization of surgical castration could help reduce health care expenditures. With rising health care costs, patients and physicians need to be aware of treatment options and their financial implications.
Keywords: Androgen deprivation therapy; Health care costs; Hormonal therapy.
Copyright © 2019 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure
Y. Zakharia reports advisory board for Amgen, Roche Diagnostics, Novartis, Jansen, Eisai, Exelixis, Castle Bioscience, Array, Bayer, Pfizer, Clovis, and EMD Serono; grant/research support (institution clinical trial support) from NewLink Genetics, Pfizer, Exelixis, and Eisai; and DSMC from Jansen. The remaining authors have stated that they have no conflicts of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68: 7–30. - PubMed
-
- United States Preventive Task Force. Screening for prostate cancer: US Preventive Services Task Force recommendation statement. JAMA 2018; 319:1901–13. - PubMed
-
- Vogelzang NJ, Chodak GW, Soloway MS, et al. Goserelin versus orchiectomy in the treatment of advanced prostate cancer: final results of a randomized trial. Urology 1995; 46:220–6. - PubMed
-
- Parmar H, Edwards L, Phillips RH, Allen L, Lightman SL. Orchiectomy versus long-acting D-Trp-6-LHRH in advanced prostatic cancer. Br J Urol 1987; 59:248–54. - PubMed
-
- Niraula S, Le LW, Tannock IF. Treatment of prostate cancer with intermittent versus continuous androgen deprivation: a systematic review of randomized trials. J Clin Oncol 2013; 31:2029–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
