

Visual Acuity and Foveal Structure in Eyes with Fragmented Foveal Avascular Zones
- PMID: 31956075
- PMCID: PMC7211138
- DOI: 10.1016/j.oret.2019.11.014
Visual Acuity and Foveal Structure in Eyes with Fragmented Foveal Avascular Zones
Abstract
Purpose: To assess the frequency and impact of abnormal foveal avascular zone (FAZ) topography (i.e., a fragmented FAZ) on visual acuity and foveal anatomic features.
Design: Prospective, cross-sectional study from March 2018 through July 2019.
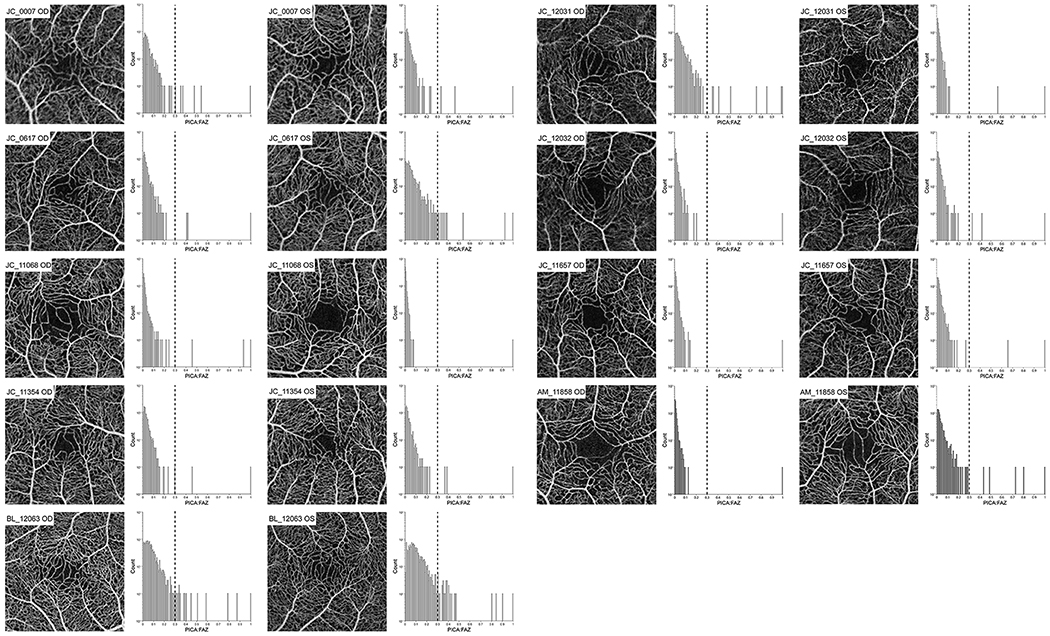
Participants: Two-hundred fifty participants were screened from a normative OCT angiography database. Of those, 12 participants were found to have at least 1 eye with a fragmented FAZ. Eight returned for follow-up imaging, along with an additional 3 participants with ocular disease (amblyopia, autosomal recessive bestrophinopathy, premature birth) having a similar FAZ phenotype.
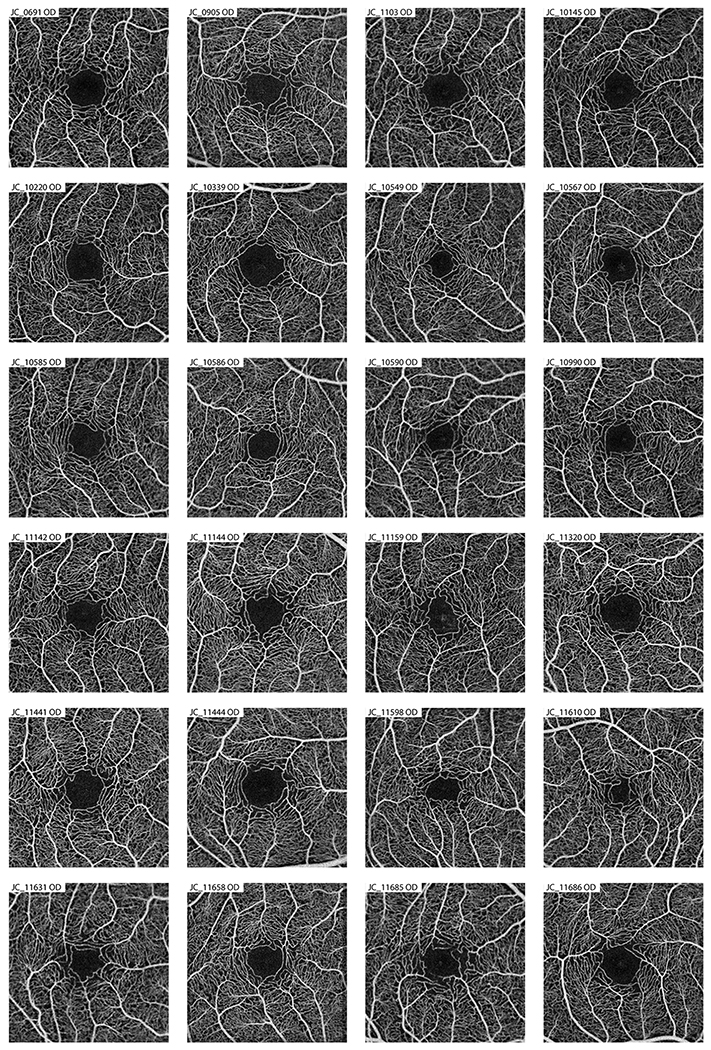
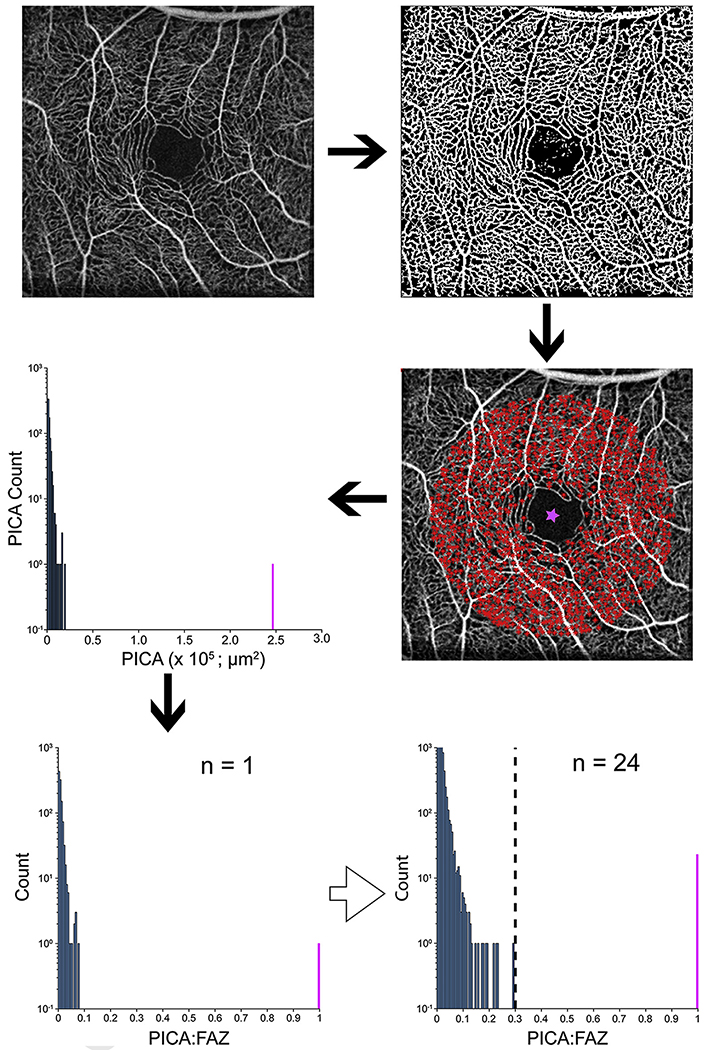
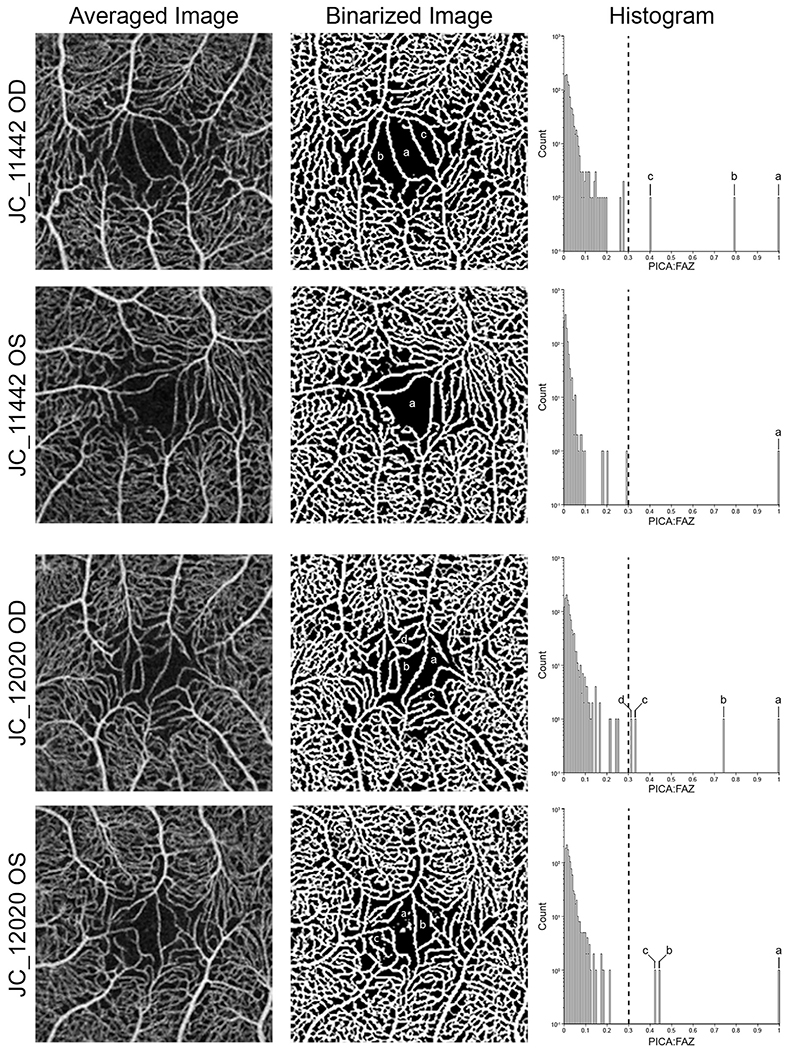
Methods: Follow-up OCT imaging and monocular best-corrected visual acuity (BCVA) were performed for these 11 participants. Twenty-four participants with a clearly defined FAZ were recruited for comparison. A normative database was created measuring parafoveal intercapillary area (PICA) to determine if an FAZ was fragmented.
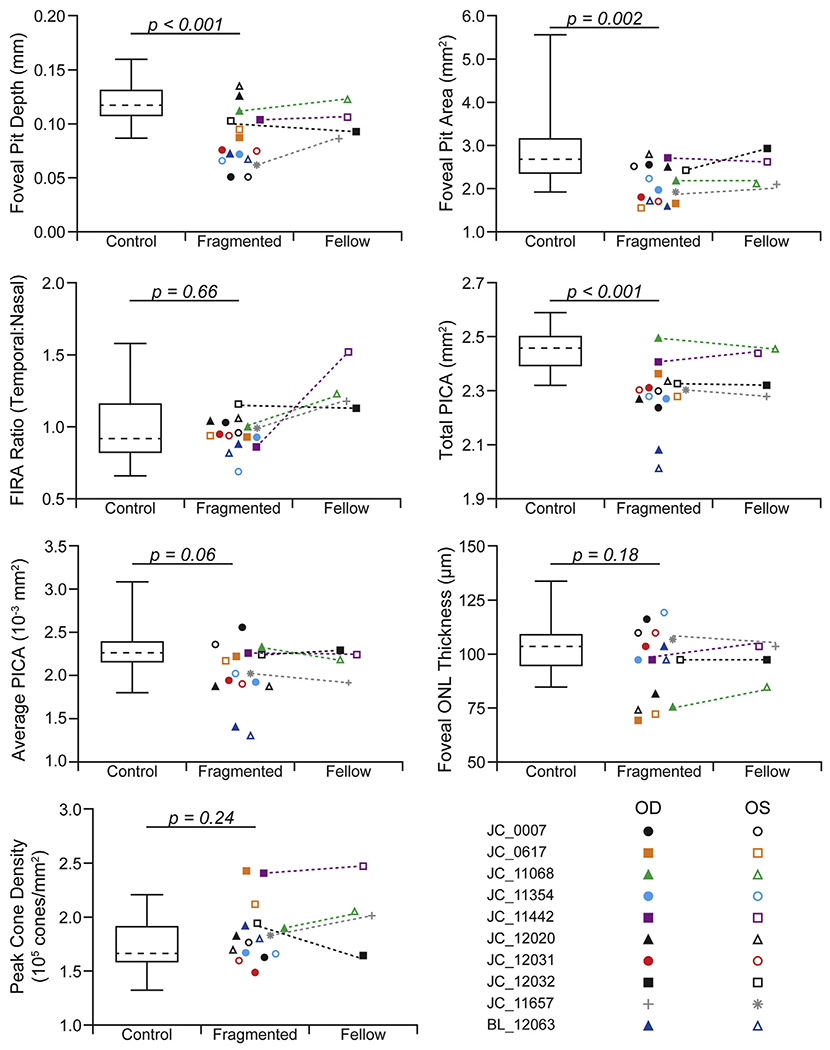
Main outcome measures: Monocular BCVA, foveal pit depth, foveal pit area, PICA, outer nuclear layer thickness, foveal inner retinal area, and peak cone density.
Results: The frequency of a fragmented FAZ was 4.8% of individuals (12 of 250) or 3.6% of eyes (18 of 500 eyes). A significant difference was found between the control eyes and eyes with fragmented FAZs for foveal pit depth, pit area, and total PICA (P < 0.001, P = 0.002, and P < 0.001, respectively). The presence of a fragmented FAZ did not affect visual acuity.
Conclusions: The presence of a fragmented FAZ seems not to be a rare phenotype in individuals with normal vision. The presence of altered FAZ topography in patients with retinal or systemic disease could negatively impact the accuracy and sensitivity of biomarkers dependent on FAZ identification.
Copyright © 2019 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Provis JM. Development of the primate retinal vasculature. Prog Retin Eye Res. 2001;20:799–821. - PubMed
-
- Tick S, Rossant F, Ghorbel I, et al. Foveal shape and structure in a normal population. Invest Ophthalmol Vis Sci. 2011;52:5105–5110. - PubMed
-
- Spaide RF, Klancnik JMJ, Cooney MJ. Retinal vascular layers in macular telangiectasia type 2 imaged by optical coherence tomography angiography. JAMA Ophthalmol. 2015;133:66–73. - PubMed
-
- Matsushita I, Nagata T, Hayashi T, et al. Foveal hypoplasia in patients with Stickler syndrome. Ophthalmology. 2017;124:896–902. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
