

Coil Embolization for Unruptured Intracranial Aneurysms at the Dawn of Stent Era: Results of the Japanese Registry of Neuroendovascular Therapy (JR-NET) 3
- PMID: 31956171
- PMCID: PMC7040433
- DOI: 10.2176/nmc.st.2019-0210
Coil Embolization for Unruptured Intracranial Aneurysms at the Dawn of Stent Era: Results of the Japanese Registry of Neuroendovascular Therapy (JR-NET) 3
Abstract
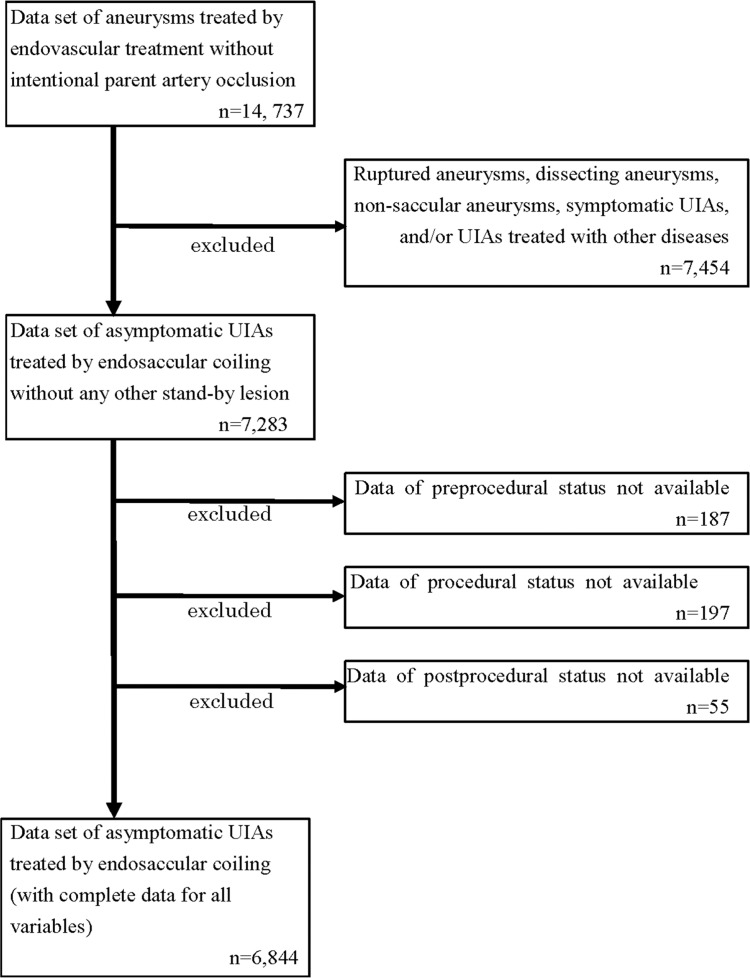
Endosaccular coiling is recognized as a feasible method for treating unruptured intracranial aneurysms (UIAs). We retrospectively reviewed cases of UIAs treated by coiling in the Japanese Registry of Neuroendovascular Therapy (JR-NET) 3, a nationwide survey of NET between 2010 and 2014, the beginning period of intracranial stents in Japan. Data were extracted for 6844 UIAs (6619 procedures) from 40,169 registered records of all NETs in the JR-NET 3 databases. The features of the aneurysms and procedures, immediate radiographic findings, procedure-related complications, and clinical outcomes at 30 days after the procedures were assessed. Of 6844 UIAs, 81.8% were located in the anterior circulation. The mean patient age was 61.3 years (72.4% females). Compared with the preceding JR-NET 1 and 2, there were significant increases (P <0.05) in the rates of the following in JR-NET 3: wide-necked and small UIAs measuring <10 mm (from 56.4% to 58.8%), adjunctive techniques (54.8% to 71.8%), and stent usage (1.1% to 22.1%). Both pre- (85.6% to 96.7%) and post-procedural (84.0% to 94.6%) antiplatelet therapy were more frequently administered in JR-NET 3. Although procedure-related complication rates did not differ between the two groups, ischemic complication rates increased from 4.6% to 5.9%, leading to an increase in the 30-day morbidity (modified Rankin Scale >2) from 2.1% to 2.8%. In conclusion, introduction of neck-bridge stent was associated with an increase in cases of wide-necked aneurysms. However, the ischemic complication rate increased despite the greater use of periprocedural antiplatelet therapy.
Keywords: Japanese Registry of Neuroendovascular Therapy; coil embolization; unruptured intracranial aneurysms.
Conflict of interest statement
Dr. Sakai received Speakers’ Bureau/Honoraria from Otsuka Pharmaceutical Co., Stryker Co., Medtronic Co, Medico’s Hirata Co., and Biomedical Solutions Co., and research funding from Otsuka Pharmaceutical Co., Terumo Co., and Daiichi Sankyo Co. Dr. Iihara received Speakers’ Bureau/Honoraria from Otsuka Pharmaceutical Co., and research funding from Otsuka Pharmaceutical Co, Mitsubishi Tanabe Pharma Co., Kaneka Medix Co., Chugai Pharmaceutical Co., and Eisai Co. Dr. Satow, Dr. Ikeda and Dr. Takahashi have no conflicts of interest to declare. All authors who are members and non-members of The Japan Neurosurgical Society (JNS) have registered self-reported COI disclosure statements through the website for JNS. This manuscript has not been published or presented elsewhere in part or in entirety, and is not under consideration by another journal.
Figures
References
-
- Sonobe M, Yamazaki T, Yonekura M, Kikuchi H: Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke 41: 1969–1977, 2010 - PubMed
-
- UCAS Japan Investigators. Morita A, Kirino T, et al. : The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med 366: 2474–2482, 2012 - PubMed
-
- Greving JP, Wermer MJ, Brown RD, et al. : Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol 13: 59–66, 2014 - PubMed
-
- Lin N, Cahill KS, Frerichs KU, Friedlander RM, Claus EB: Treatment of ruptured and unruptured cerebral aneurysms in the USA: a paradigm shift. J Neurointerv Surg 4: 182–189, 2012 - PubMed