

How I treat cancer-associated thrombosis
- PMID: 31958288
- PMCID: PMC7003382
- DOI: 10.1136/esmoopen-2019-000610
How I treat cancer-associated thrombosis
Abstract
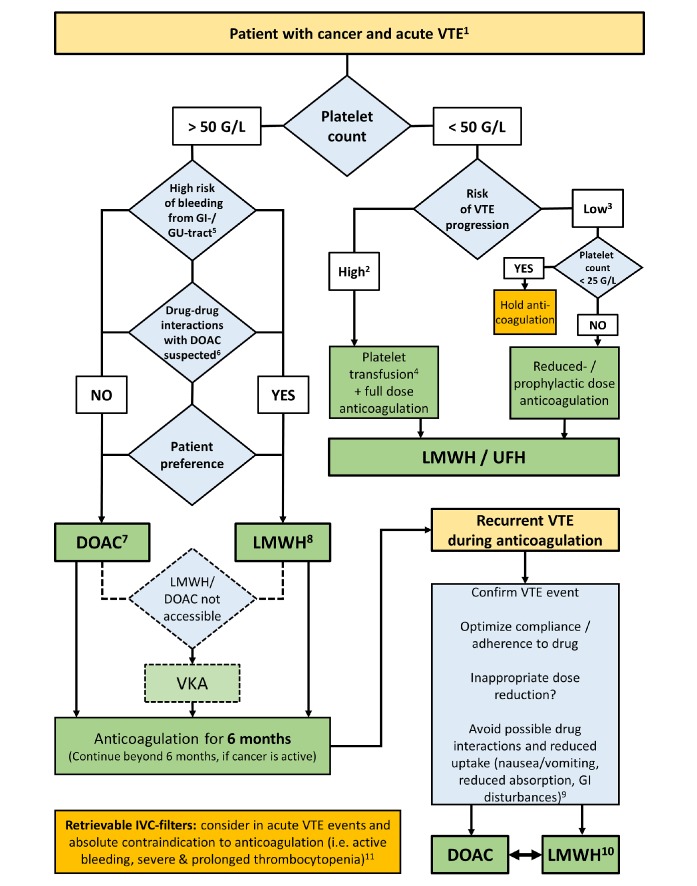
Patients with cancer are at an increased risk of symptomatic venous thromboembolism (VTE). In addition, an increasing number of patients with incidental thromboembolic events have been recorded in clinical practice. Therapeutic anticoagulation is crucial to prevent thrombus progression and reduce risk of recurrence; however, this comes at the price of an increased bleeding risk, which necessitates a personalised approach to choose the most appropriate type of therapy. Over the last decade, low-molecular-weight heparin has been the preferred anticoagulant agent for patients with cancer-associated thrombosis due to better efficacy and similar safety profile compared with vitamin K antagonists. While direct oral anticoagulants (DOAC) have emerged as new option for treatment of VTE in a general population, only limited data have been available specifically for patients with cancer until recently. Randomised, controlled trials have now been published, establishing DOAC as an alternative for the treatment of cancer-associated thrombosis. However, the improvement in the therapeutic armamentarium is accompanied by a number of special considerations. For instance, risk of bleeding is elevated in patients with cancer-associated VTE receiving DOAC, especially in certain tumour types (eg, gastrointestinal), and no guidance exists regarding their use in patients with severe thrombocytopaenia. Furthermore, DOAC are prone to certain drug-drug interactions and their effect might be altered due to nausea and vomiting in patients receiving chemotherapy. Here, we provide guidance on how to treat cancer-associated VTE and how new evidence from randomised controlled trials can be implemented in clinical practice. There are still clinical scenarios where robust evidence is lacking and treatment recommendations are based on extrapolations from other populations or expert opinion only. Therefore, additional research in special subpopulations is needed to optimise management of patients in challenging clinical scenarios.
Keywords: anticoagulation; cancer; direct oral anticoagulants; thrombosis; venous thromboembolism.
© Author (s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ on behalf of the European Society for Medical Oncology.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
