

A Geographic Analysis of Racial Disparities in Use of Pulmonary Rehabilitation After Hospitalization for COPD Exacerbation
- PMID: 31958438
- PMCID: PMC7242634
- DOI: 10.1016/j.chest.2019.11.044
A Geographic Analysis of Racial Disparities in Use of Pulmonary Rehabilitation After Hospitalization for COPD Exacerbation
Abstract
Background: Guidelines recommend pulmonary rehabilitation (PR) after hospitalization for an exacerbation of COPD, but few patients enroll in PR. We explored whether density of PR programs explained regional variation and racial disparities in receipt of PR.
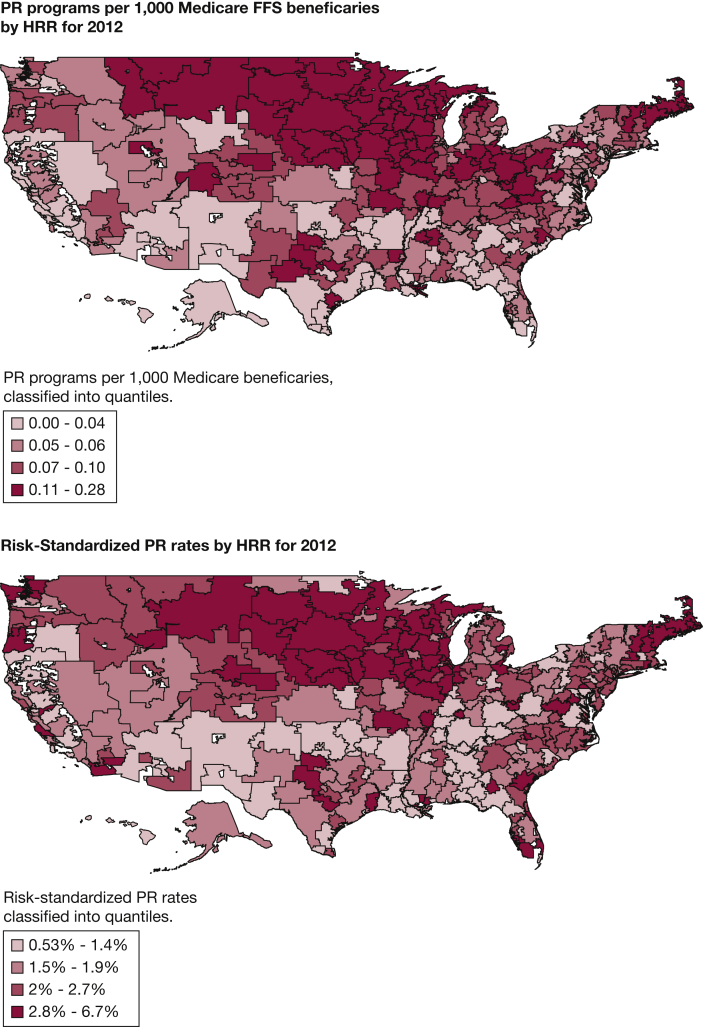
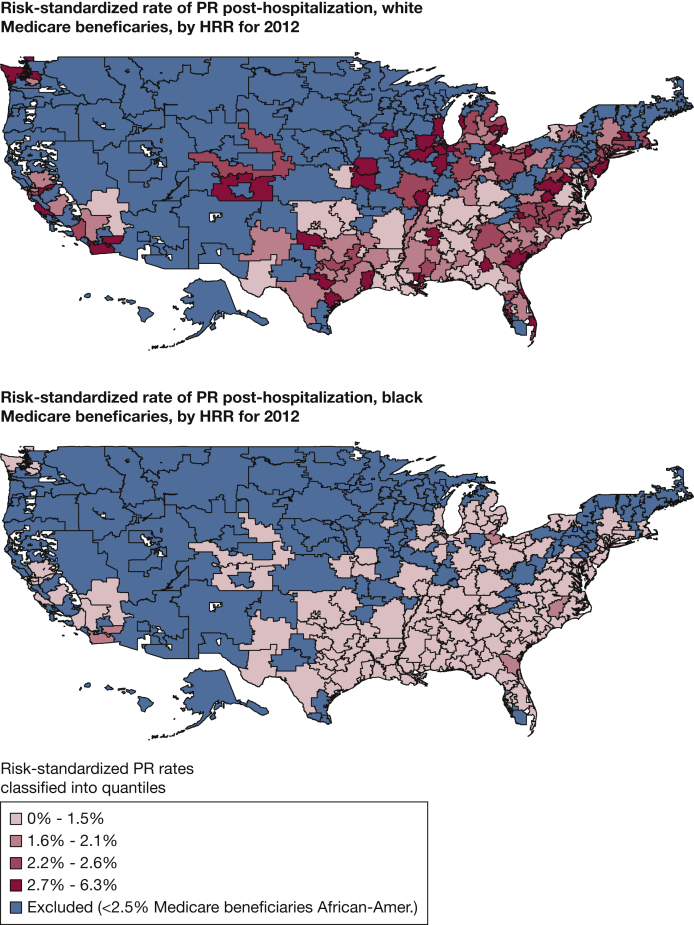
Methods: We used Centers for Medicare & Medicaid Services data from 223,832 Medicare beneficiaries hospitalized for COPD during 2012 who were eligible for PR postdischarge. We used Hospital-Referral Regions (HRR) as the unit of analysis. For each HRR, we calculated the density of PR programs as a measure of program access and estimated risk-standardized rates of PR within 6 months of discharge overall, and for non-Hispanic, white, and black beneficiaries. We used linear regression to examine the relationship between access to PR and HRR PR rates. We tested for racial disparity in PR rates among non-Hispanic white and black beneficiaries living in the same HRRs.
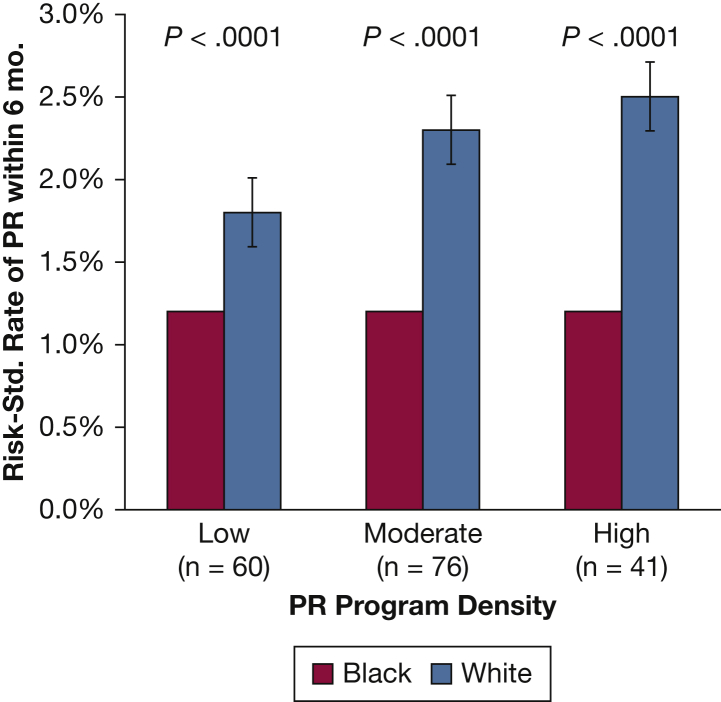
Results: Across 306 HRRs, the median number of PR programs per 1,000 Medicare beneficiaries was 0.06 (interquartile range [IQR], 0.04-0.10). Risk-standardized rates of PR ranged from 0.53% to 6.67% (median, 1.93%). Density of PR programs was positively associated with PR rates overall and among non-Hispanic white beneficiaries (P < .001), but this relationship was not observed among black beneficiaries. Rates were higher among non-Hispanic white beneficiaries (median, 2.08%; IQR, 1.54%-2.87%) compared with black beneficiaries (median, 1.19%; IQR, 1.15%-1.20%).
Conclusions: Greater PR program density was associated with higher rates of PR for non-Hispanic white but not black beneficiaries. Further research is needed to identify reasons for this discrepancy and strategies to increase receipt of PR for black patients.
Keywords: Medicare; geographic analysis; pulmonary disease, chronic obstructive; pulmonary rehabilitation; racial disparties.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Racial Disparities: Another Important Barrier to Pulmonary Rehabilitation Participation in Patients With COPD Posthospitalization.Chest. 2020 May;157(5):1070-1072. doi: 10.1016/j.chest.2020.01.029. Chest. 2020. PMID: 32386631 No abstract available.
-
Racial Disparities in Pulmonary and Critical Care Medicine.Am J Respir Crit Care Med. 2022 May 15;205(10):1236. doi: 10.1164/rccm.202106-1464RR. Am J Respir Crit Care Med. 2022. PMID: 35286240 No abstract available.
References
-
- National Heart, Lung, and Blood Institute What Is COPD? National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health/health-topics/topics/copd/# Published April 28, 2017. Accessed November 29, 2017.
-
- COPD Costs. Centers for Disease Control and Prevention. https://www.cdc.gov/copd/pubs/COPD-2014-Cost-Infographic-h.pdf
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
