Elevated Neutrophil to Lymphocyte Ratio in Older Adults with Cocaine Use Disorder as a Marker of Chronic Inflammation
- PMID: 31958903
- PMCID: PMC7006975
- DOI: 10.9758/cpn.2020.18.1.32
Elevated Neutrophil to Lymphocyte Ratio in Older Adults with Cocaine Use Disorder as a Marker of Chronic Inflammation
Abstract
Objective: The neutrophil to lymphocyte ratio (NLR) is a non-specific, easy-to-obtain marker of inflammation associated with morbidity and mortality in systemic, psychiatric, and age-related inflammatory conditions. Given the growing trend of substance use disorder (SUD) in older adults, and the relationship between inflammation and SUD elevated NLR may serve as a useful inflammatory biomarker of the combined burden of aging and SUD. The present study focused on cocaine use disorder (CUD) to examine if cocaine adds further inflammatory burden among older adults, by comparing NLR values between older adults with CUD and a non-cocaine using, aged-matched, nationally representative sample.
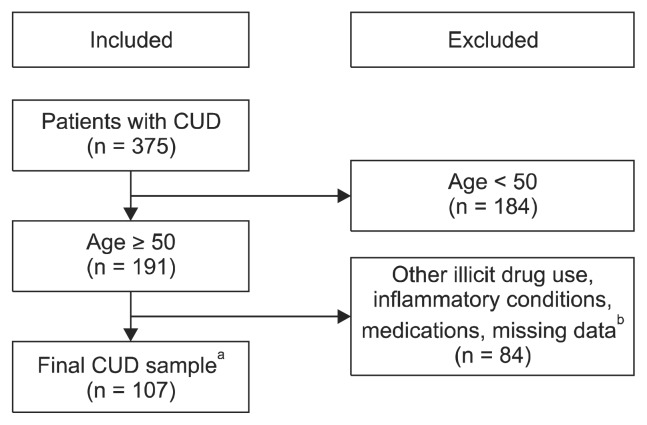
Methods: The dataset included 107 (86% male) participants (aged 50-65 years) with cocaine use disorder. NLR was derived from complete blood count tests by dividing the absolute value of peripheral neutrophil concentration by lymphocyte concentration. For comparison, we extracted data from age-matched adults without CUD using the National Health and Nutrition Examination Survey. Individuals with immunocompromising conditions were excluded (e.g., rheumatoid arthritis and sexually transmitted infections such as HIV). A doubly-robust inverse probability-weighted regression adjustment (IPWRA) propensity score method was used to estimate group differences on NLR while controlling for potential confounding variables (age, gender, race, income, nicotine, marijuana and alcohol use).
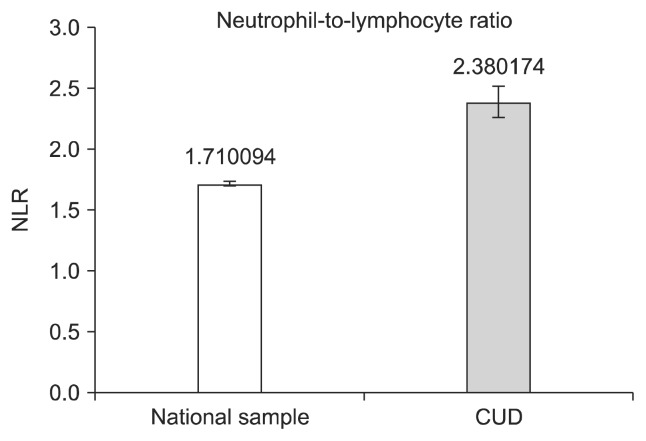
Results: The IPWRA model revealed that the CUD sample had significantly elevated NLR in comparison to non-cocaine users, with a moderate effect size (β weight = 0.67).
Conclusion: Although non-specific, NLR represents a readily obtainable inflammatory marker for SUD research. CUD may add further inflammatory burden to aging cocaine users.
Keywords: Aging; Cocaine; Inflammation; Lymphocytes; Neutrophils..
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources