

Prognostic Significance of Left Ventricular Noncompaction: Systematic Review and Meta-Analysis of Observational Studies
- PMID: 31959004
- PMCID: PMC7012350
- DOI: 10.1161/CIRCIMAGING.119.009712
Prognostic Significance of Left Ventricular Noncompaction: Systematic Review and Meta-Analysis of Observational Studies
Abstract
Background: Although left ventricular noncompaction (LVNC) has been associated with an increased risk of adverse cardiovascular events, the accurate incidence of cardiovascular morbidity and mortality is unknown. We, therefore, aimed to assess the incidence rate of LVNC-related cardiovascular events.
Methods: We systematically searched observational studies reporting the adverse outcomes related to LVNC. The primary end point was cardiovascular mortality.
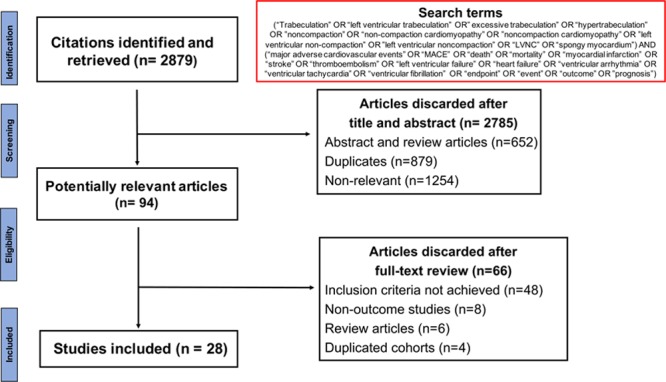
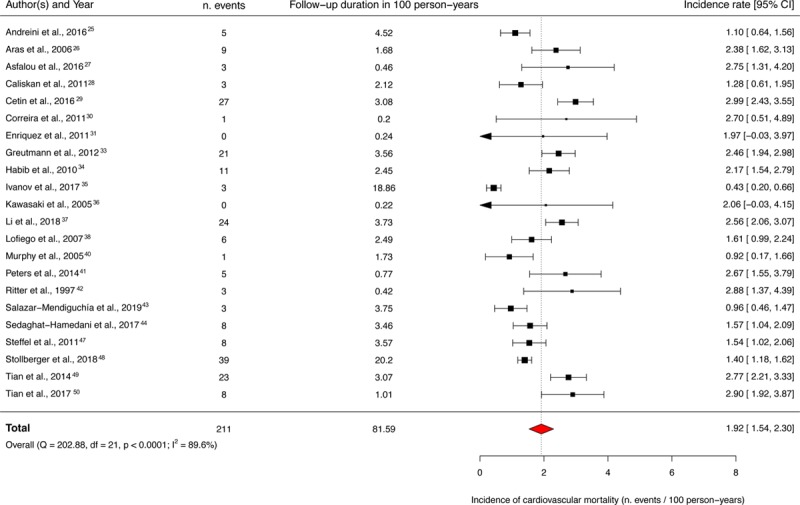
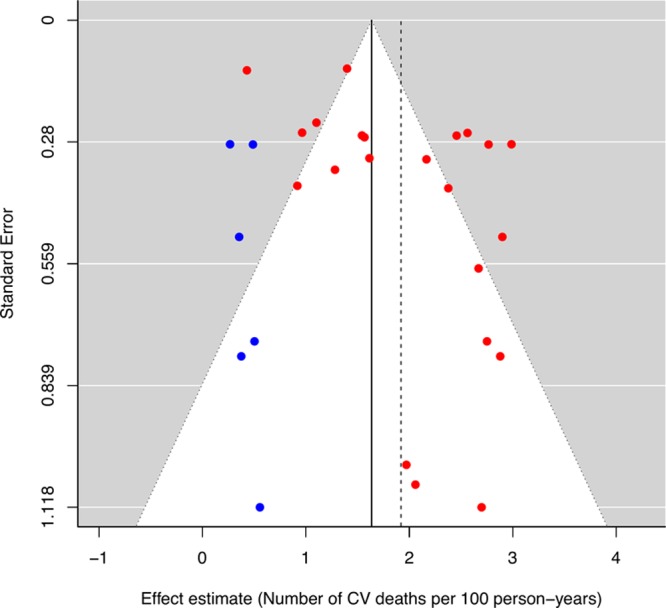
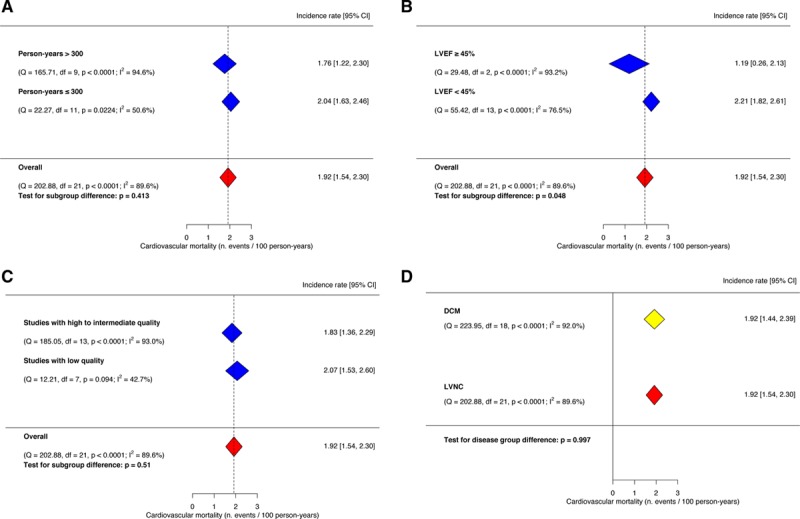
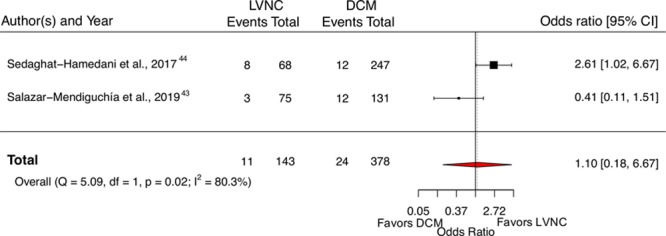
Results: We identified 28 eligible studies enrolling 2501 LVNC patients (mean age, 46 years; male/female ratio, 1.7). After a median follow-up of 2.9 years, the pooled event rate for cardiovascular mortality was 1.92 (95% CI, 1.54-2.30) per 100 person-years. LVNC patients had a similar risk of cardiovascular mortality compared with a dilated cardiomyopathy control group (odds ratio, 1.10 [95% CI, 0.18-6.67]). The incidence rates of all-cause mortality, stroke and systemic emboli, heart failure admission, cardiac transplantation, ventricular arrhythmias, and cardiac device implantation were 2.16, 1.54, 3.53, 1.24, 2.17, and 2.66, respectively, per 100 person-years. Meta-regression and subgroup analyses revealed that left ventricular ejection fraction, not the extent of left ventricular trabeculation, had an important influence on the variability of incidence rates. The risks of thromboembolism and ventricular arrhythmias in LVNC patients were similar to dilated cardiomyopathy patients. However, LVNC patients had a higher incidence of heart failure hospitalization than dilated cardiomyopathy patients.
Conclusions: Patients with LVNC carry a similar cardiovascular risk when compared with dilated cardiomyopathy patients. Left ventricular ejection fraction-a conventional indicator of heart failure severity, not the extent of trabeculation-appears to be an important determinant of adverse outcomes in LVNC patients. Registration: https://www.crd.york.ac.uk/PROSPERO/ Unique identifier: CRD42018096313.
Keywords: cardiac imaging techniques; cardiomyopathies; meta-analysis; prognosis.
Figures
Comment in
-
Outcomes in Left Ventricular Noncompaction: Heterogeneity in Results or Heterogeneity in Diagnosing a Heterogeneous Disease?Circ Cardiovasc Imaging. 2020 Jan;13(1):e010268. doi: 10.1161/CIRCIMAGING.119.010268. Epub 2020 Jan 21. Circ Cardiovasc Imaging. 2020. PMID: 31959005 No abstract available.
References
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman CE, Young JB American Heart Association. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. - PubMed
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P, Dubourg O, Kühl U, Maisch B, McKenna WJ, et al. Classification of the cardiomyopathies: a position statement from the European Society Of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2008;29:270–276. doi: 10.1093/eurheartj/ehm342. - PubMed
-
- Gati S, Chandra N, Bennett RL, Reed M, Kervio G, Panoulas VF, Ghani S, Sheikh N, Zaidi A, Wilson M, et al. Increased left ventricular trabeculation in highly trained athletes: do we need more stringent criteria for the diagnosis of left ventricular non-compaction in athletes? Heart Br Card Soc. 2013;99:401–408. doi: 10.1136/heartjnl-2012-303418. - PubMed
-
- Gati S, Papadakis M, Van Niekerk N, Reed M, Yeghen T, Sharma S. Increased left ventricular trabeculation in individuals with sickle cell anaemia: physiology or pathology? Int J Cardiol. 2013;168:1658–1660. doi: 10.1016/j.ijcard.2013.03.039. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
