

Cryptococcal antigenemia is associated with meningitis or death in HIV-infected adults with CD4 100-200 cells/mm3
- PMID: 31959112
- PMCID: PMC6971851
- DOI: 10.1186/s12879-020-4798-1
Cryptococcal antigenemia is associated with meningitis or death in HIV-infected adults with CD4 100-200 cells/mm3
Abstract
Background: Cryptococcal antigen (CrAg) screening with fluconazole prophylaxis has been shown to prevent cryptococcal meningitis and mortality for people living with HIV (PLWH) with CD4 < 100 cells/mm3. While cryptococcal meningitis occurs in individuals with CD4 100-200 cells/mm3, there is limited evidence that CrAg screening predicts cryptococcal meningitis or mortality among this group with moderate immunosuppression. Current IDSA and WHO clinical guidelines recommend restricting CrAg screening to PLWH with CD4 < 100 cells/mm3.
Methods: We conducted a prospective cohort study of PLWH 18+ years who had not initiated ART in South Africa. We followed participants for 14 months to determine onset of cryptococcal meningitis or all-cause mortality. At study completion, we retrospectively tested stored serum samples for CrAg using an enzyme immunoassay (EIA). We calculated CD4-stratified incidence rates of outcomes and used Cox proportional hazards to measure associations between CrAg positivity and outcomes.
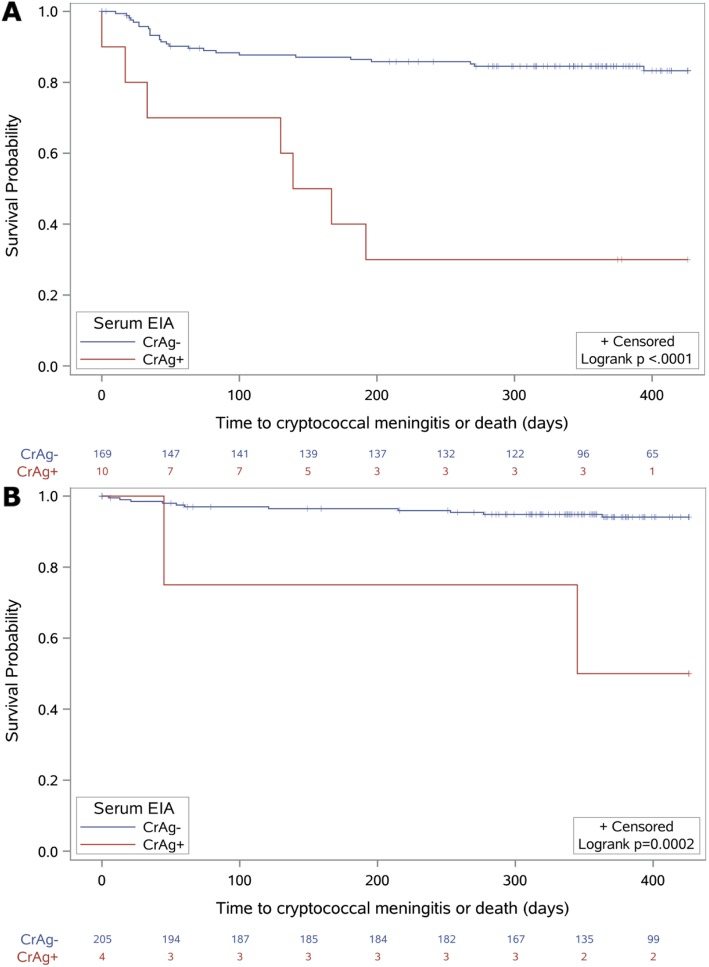
Results: We enrolled 2383 PLWH, and 1309 participants had serum samples tested by CrAg EIA. The median CD4 was 317 cells/mm3 (interquartile range: 173-491 cells/mm3). By CD4 count at baseline, there were 209 individuals with a CD4 count of 100-200 cells/mm3 and available CrAg test results. Of these, four (1.9%) tested positive. Two of four (IR: 58.8 per 100 person-years) CrAg+ participants and 11 of 205 (IR: 5.6 per 100 person-years) CrAg- participants developed cryptococcal meningitis or died for an overall rate of death or cryptococcal meningitis that was 10.0-times higher for those who were CrAg+ (95% confidence interval: 2.2-45.3). Among those with CD4 < 100 cell/mm3 and CrAg EIA test results (N = 179), ten (5.6%) participants tested CrAg+. Among this group, seven of ten (IR: 137.6 per 100 person-years) CrAg+ participants and 26 of 169 (IR: 17.8 per 100 person-years) CrAg- participants developed cryptococcal meningitis or died, for a rate of death or cryptococcal meningitis that was 6.3-times higher for those who were CrAg+ (95% confidence interval: 2.7-14.6).
Conclusions: Although few PLWH with moderate immunosuppression screened CrAg positive, a positive CrAg test was predictive of increased risk of cryptococcal meningitis or death. Similar to those with a CD4 < 100 cell/mm3, systematic CrAg screening may reduce morbidity and mortality in PLWH with CD4 100-200 cells/mm3.
Keywords: Cryptococcal antigen; Cryptococcal meningitis; HIV; Opportunistic infections; Screening; Sub-Saharan Africa.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Diagnosis THE, Cryptococcal MOF, Adults DINH. The Diagnosis, Prevention and Management of Cryptococcal Disease in Hiv-Infected Adults, Adolescents and Children Supplement To the 2016 Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing Hiv Infection 2018. - PubMed
-
- Stover J, Low A, Larke N, Drouin O, B-Lajoie M-R, Gavriilidis G, et al. Incidence of opportunistic infections and the impact of antiretroviral therapy among HIV-infected adults in Low- and middle-income countries: a systematic review and meta-analysis. Clin Infect Dis. 2016;62(12):1595–1603. doi: 10.1093/cid/ciw125. - DOI - PMC - PubMed
-
- Temfack E, Bigna JJ, Luma HN, Spijker R, Meintjes G, Jarvis JN, et al. Impact of routine Cryptococcal antigen screening and targeted preemptive fluconazole therapy in antiretroviral-naive human immunodeficiency virus-infected adults with CD4 cell counts <100/muL: a systematic review and meta-analysis. Clin Infect Dis. 2019;68(4):688–698. doi: 10.1093/cid/ciy567. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
