

Incidence and mortality from cervical cancer and other malignancies after treatment of cervical intraepithelial neoplasia: a systematic review and meta-analysis of the literature
- PMID: 31959338
- PMCID: PMC7479506
- DOI: 10.1016/j.annonc.2019.11.004
Incidence and mortality from cervical cancer and other malignancies after treatment of cervical intraepithelial neoplasia: a systematic review and meta-analysis of the literature
Abstract
Background: Although local treatments for cervical intraepithelial neoplasia (CIN) are highly effective, it has been reported that treated women remain at increased risk of cervical and other cancers. Our aim is to explore the risk of developing or dying from cervical cancer and other human papillomavirus (HPV)- and non-HPV-related malignancies after CIN treatment and infer its magnitude compared with the general population.
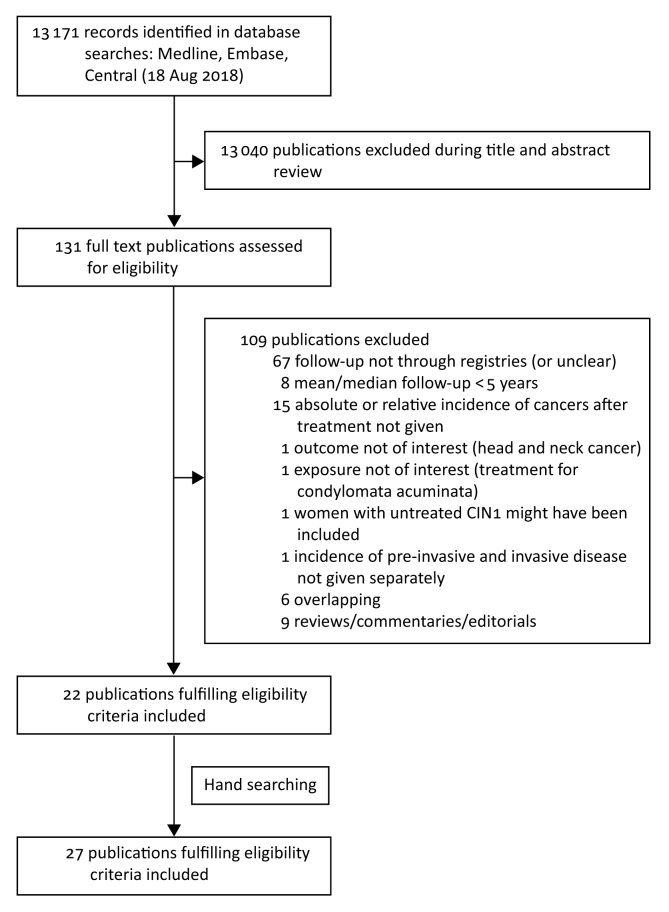
Materials and methods: Design: Systematic review and meta-analysis. Eligibility criteria: Studies with registry-based follow-up reporting cancer incidence or mortality after CIN treatment.
Data synthesis: Summary effects were estimated using random-effects models.
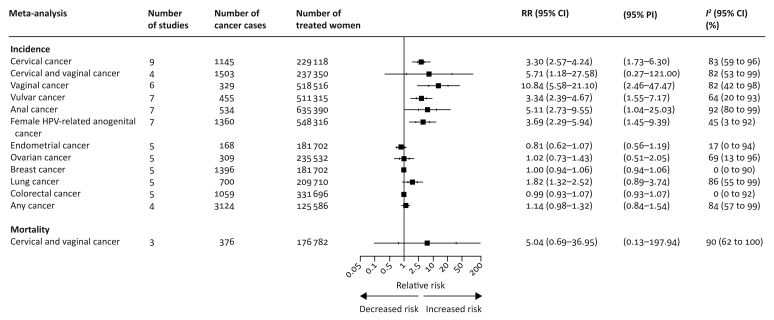
Outcomes: Incidence rate of cervical cancer among women treated for CIN (per 100 000 woman-years). Relative risk (RR) of cervical cancer, other HPV-related anogenital tract cancer (vagina, vulva, anus), any cancer, and mortality, for women treated for CIN versus the general population.
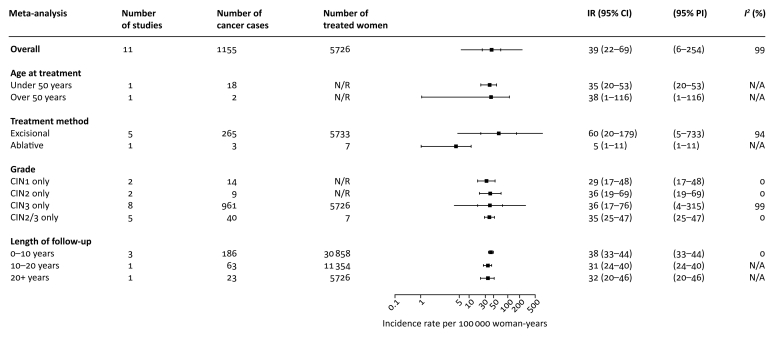
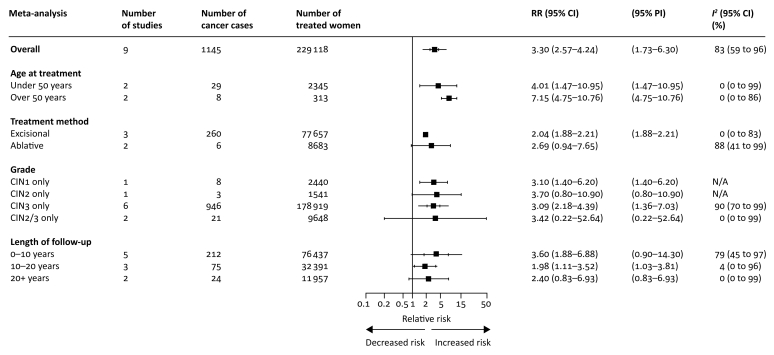
Results: Twenty-seven studies were eligible. The incidence rate for cervical cancer after CIN treatment was 39 per 100 000 woman-years (95% confidence interval 22-69). The RR of cervical cancer was elevated compared with the general population (3.30, 2.57-4.24; P < 0.001). The RR was higher for women more than 50 years old and remained elevated for at least 20 years after treatment. The RR of vaginal (10.84, 5.58-21.10; P < 0.001), vulvar (3.34, 2.39-4.67; P < 0.001), and anal cancer (5.11, 2.73-9.55; P < 0.001) was also higher. Mortality from cervical/vaginal cancer was elevated, but our estimate was more uncertain (RR 5.04, 0.69-36.94; P = 0.073).
Conclusions: Women treated for CIN have a considerably higher risk to be later diagnosed with cervical and other HPV-related cancers compared with the general population. The higher risk of cervical cancer lasts for at least 20 years after treatment and is higher for women more than 50 years of age. Prolonged follow-up beyond the last screening round may be warranted for previously treated women.
Keywords: CIN; HPV-related cancer; LLETZ; cancer incidence; cancer mortality; conisation.
Copyright © 2019 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Evidence for the path to cervical cancer elimination.Lancet Glob Health. 2020 Feb;8(2):e155-e156. doi: 10.1016/S2214-109X(19)30523-6. Epub 2019 Dec 4. Lancet Glob Health. 2020. PMID: 31812370 No abstract available.
References
-
- Canfell K., Sitas F., Beral V. Cervical cancer in Australia and the United Kingdom: comparison of screening policy and uptake, and cancer incidence and mortality. Med J Aust. 2006;185:482–486. - PubMed
-
- Arbyn M., Redman C.W.E., Verdoodt F. Incomplete excision of cervical precancer as a predictor of treatment failure: a systematic review and meta-analysis. Lancet Oncol. 2017;18:1665–1679. - PubMed
-
- Jakobsson M., Gissler M., Paavonen J., Tapper A.M. Long-term mortality in women treated for cervical intraepithelial neoplasia. BJOG. 2009;116:838–844. - PubMed
