

Clustering of health, crime and social-welfare inequality in 4 million citizens from two nations
- PMID: 31959926
- PMCID: PMC7082196
- DOI: 10.1038/s41562-019-0810-4
Clustering of health, crime and social-welfare inequality in 4 million citizens from two nations
Abstract
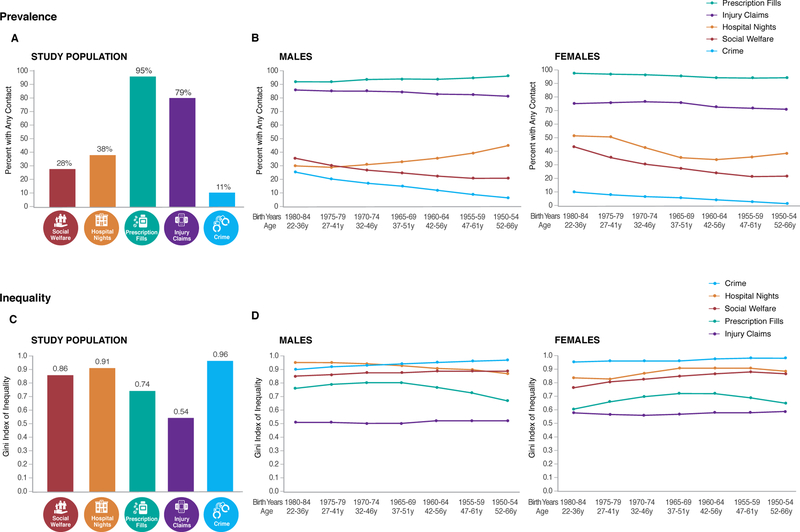
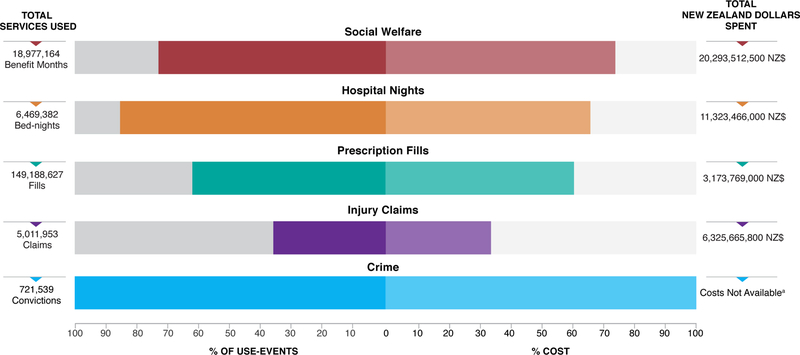
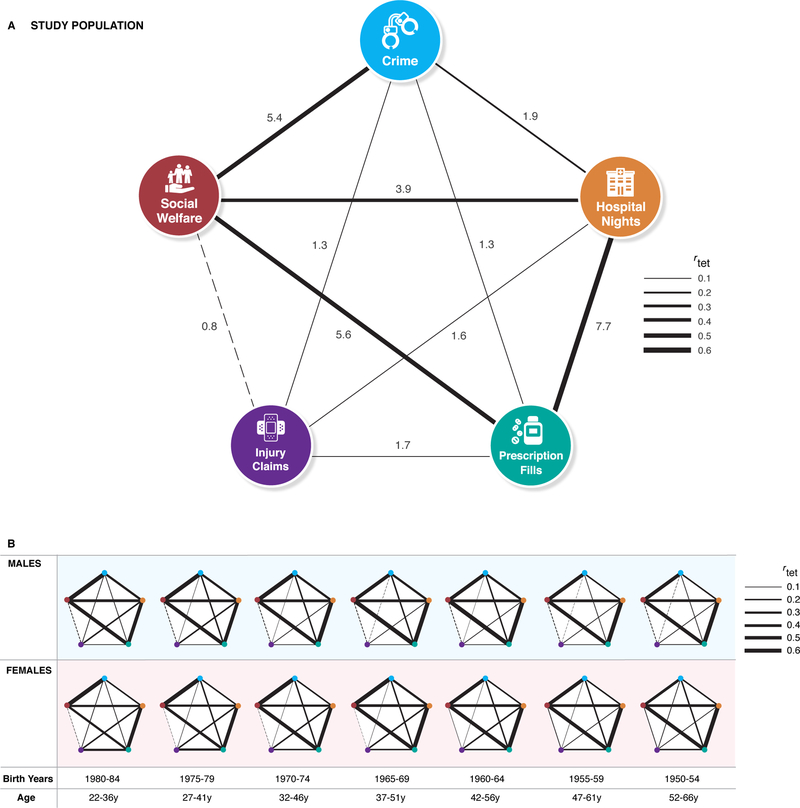
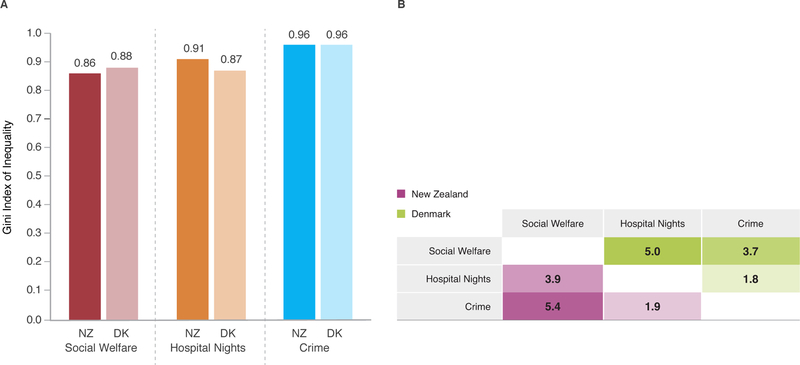
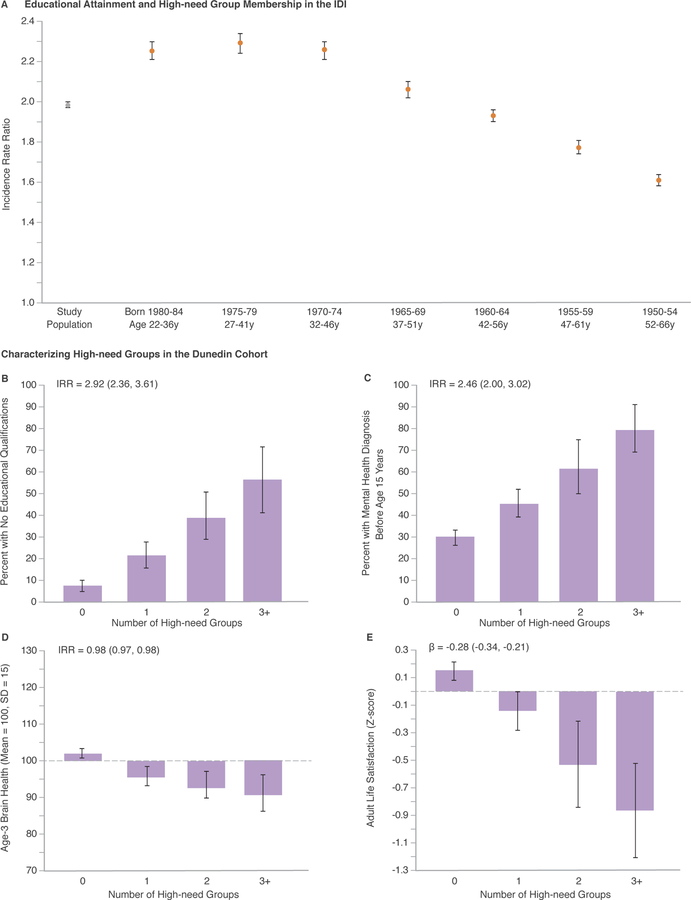
Health and social scientists have documented the hospital revolving-door problem, the concentration of crime, and long-term welfare dependence. Have these distinct fields identified the same citizens? Using administrative databases linked to 1.7 million New Zealanders, we quantified and monetized inequality in distributions of health and social problems and tested whether they aggregate within individuals. Marked inequality was observed: Gini coefficients equalled 0.96 for criminal convictions, 0.91 for public-hospital nights, 0.86 for welfare benefits, 0.74 for prescription-drug fills and 0.54 for injury-insurance claims. Marked aggregation was uncovered: a small population segment accounted for a disproportionate share of use-events and costs across multiple sectors. These findings were replicated in 2.3 million Danes. We then integrated the New Zealand databases with the four-decade-long Dunedin Study. The high-need/high-cost population segment experienced early-life factors that reduce workforce readiness, including low education and poor mental health. In midlife they reported low life satisfaction. Investing in young people's education and training potential could reduce health and social inequalities and enhance population wellbeing.
Conflict of interest statement
Figures

References
-
- Alvaredo F, Chancel L, Piketty T, Saez E, Zucman C, eds. World Inequality Report 2018 (Belknap Press, 2018).
-
- International Monetary Fund. Fiscal Monitor: Tackling Inequality (IMF, October 2017).
-
- OECD; Income Inequality Update (November 2016).
-
- Keeley B. Income Inequality: the Gap Between Rich and Poor (OECD Publishing, 2015).
-
- Goodman D, Fisher E & Chang C. The Revolving Door: A Report on U.S. Hospital Readmissions (Robert Wood Johnson Foundation, 2013).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
