

Multitrait analysis of glaucoma identifies new risk loci and enables polygenic prediction of disease susceptibility and progression
- PMID: 31959993
- PMCID: PMC8056672
- DOI: 10.1038/s41588-019-0556-y
Multitrait analysis of glaucoma identifies new risk loci and enables polygenic prediction of disease susceptibility and progression
Abstract
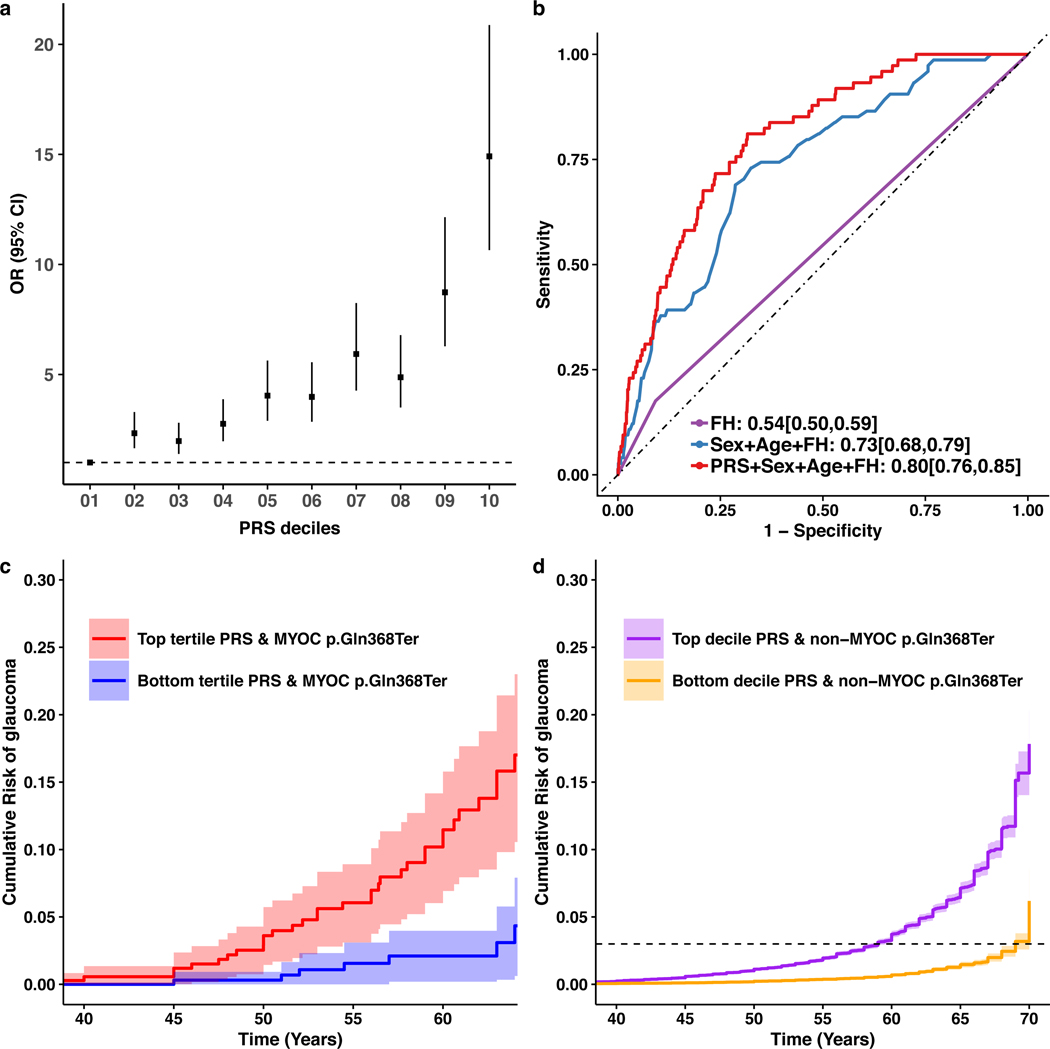
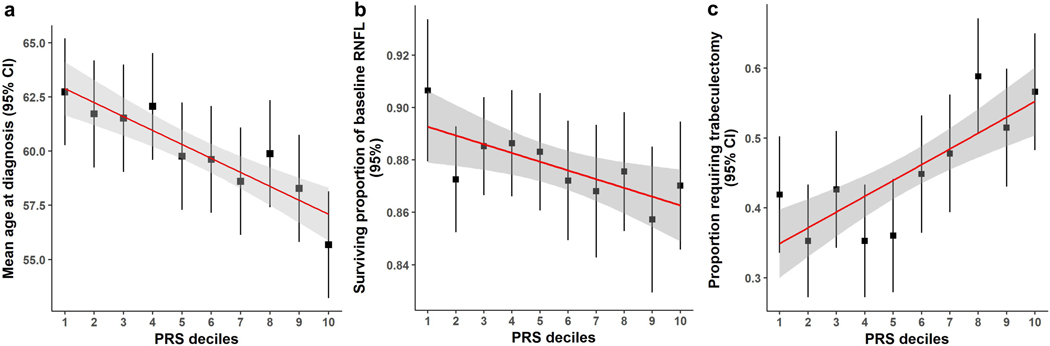
Glaucoma, a disease characterized by progressive optic nerve degeneration, can be prevented through timely diagnosis and treatment. We characterize optic nerve photographs of 67,040 UK Biobank participants and use a multitrait genetic model to identify risk loci for glaucoma. A glaucoma polygenic risk score (PRS) enables effective risk stratification in unselected glaucoma cases and modifies penetrance of the MYOC variant encoding p.Gln368Ter, the most common glaucoma-associated myocilin variant. In the unselected glaucoma population, individuals in the top PRS decile reach an absolute risk for glaucoma 10 years earlier than the bottom decile and are at 15-fold increased risk of developing advanced glaucoma (top 10% versus remaining 90%, odds ratio = 4.20). The PRS predicts glaucoma progression in prospectively monitored, early manifest glaucoma cases (P = 0.004) and surgical intervention in advanced disease (P = 3.6 × 10-6). This glaucoma PRS will facilitate the development of a personalized approach for earlier treatment of high-risk individuals, with less intensive monitoring and treatment being possible for lower-risk groups.
Figures
References
-
- Weinreb RN & Khaw PT Primary open-angle glaucoma. Lancet 363, 1711–1720 (2004). - PubMed
-
- Tham Y-C et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 121, 2081–2090 (2014). - PubMed
-
- Mitchell P, Smith W, Attebo K. & Healey PR Prevalence of open-angle glaucoma in Australia. The Blue Mountains Eye Study. Ophthalmology 103, 1661–1669 (1996). - PubMed
Methods-only References:
-
- Souzeau E. et al. Australian and New Zealand Registry of Advanced Glaucoma: methodology and recruitment. Clin. Experiment. Ophthalmol 40, 569–575 (2012). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_UU_00007/10/MRC_/Medical Research Council/United Kingdom
- MR/T040912/1/MRC_/Medical Research Council/United Kingdom
- U01 HG004728/HG/NHGRI NIH HHS/United States
- R21 EY028671/EY/NEI NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- R01 EY022305/EY/NEI NIH HHS/United States
- R01 EY015473/EY/NEI NIH HHS/United States
- MC_PC_12028/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- P30 EY014104/EY/NEI NIH HHS/United States
- P30 EY031631/EY/NEI NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
