

Review
doi: 10.1161/JAHA.119.013757.
Epub 2020 Jan 21.
Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment
Affiliations
- PMID: 31960755
- PMCID: PMC7033840
- DOI: 10.1161/JAHA.119.013757
Item in Clipboard
Review
Immune Checkpoint Inhibitor Myocarditis: Pathophysiological Characteristics, Diagnosis, and Treatment
J Am Heart Assoc.
.
No abstract available
Keywords: cardiotoxicity; immune checkpoint inhibitors; myocarditis.
Figures
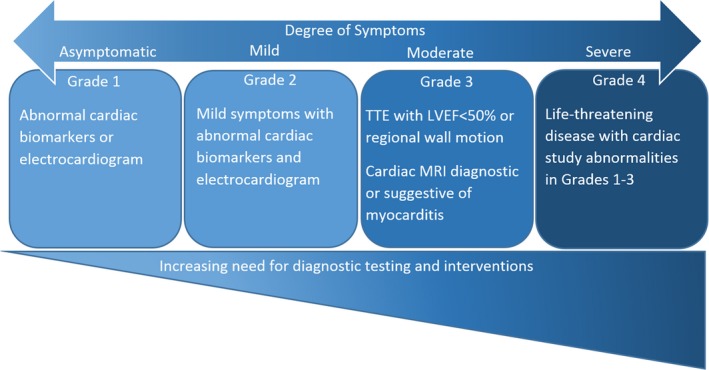
Spectrum of disease in immune checkpoint inhibitor–related myocarditis. The diagnosis of myocarditis is made after ruling out all other causes, such as ischemia or supply/demand mismatch. The grades of severity listed are from the American Society of Clinical Oncology clinical practice guidelines for the management of immune‐related adverse events (Brahmer et al23). LVEF indicates left ventricular ejection fraction; MRI, magnetic resonance imaging; TTE, transthoracic echocardiogram.
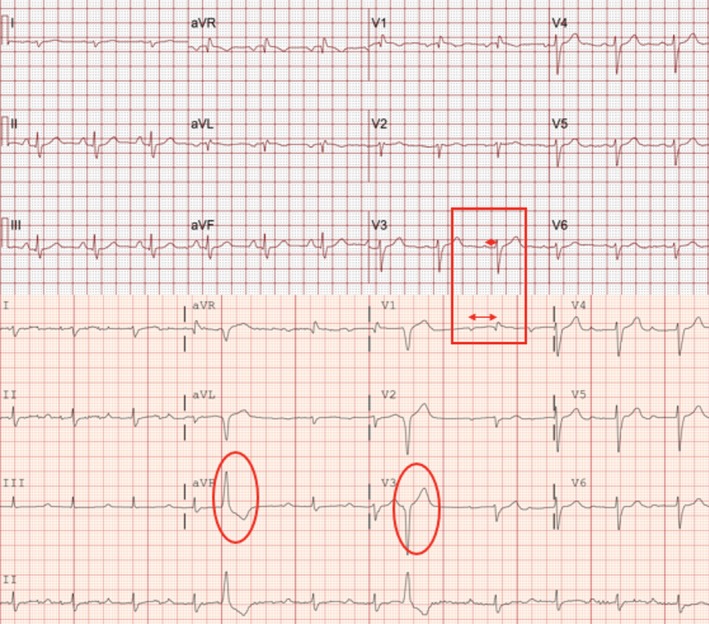
ECG abnormalities: Presented is an example of ECG abnormalities encountered during immune checkpoint inhibitor myocarditis. The severe prolongation of the PR interval on presentation can be a harbinger of potentially serious rhythm abnormalities, such as complete heart block, which occurred in this patient. Top, Baseline ECG before initiating immune checkpoint inhibitors. Normal PR interval (red box with short double arrow) and no premature ventricular complexes. Bottom, After 4 doses of nivolumab, patient presented with dyspnea and decompensated heart failure. ECG reveals new prolongation in PR interval (red box with long double arrow) and frequent premature ventricular complexes (red ovals). The patient had a temporary pacemaker placed and progressed to advanced atrioventricular block, which later recovered, and PR interval returned to normal after initiation of steroids, plasmapheresis, and infliximab.

Cardiac magnetic resonance imaging of myocarditis. This case meets updated Lake‐Louise Criteria for fibrosis and edema, which is the current definition of myocarditis by cardiac magnetic resonance imaging. Left, Late gadolinium enhancement (LGE) image of replacement fibrosis at the interventricular septum with midmyocardial distribution not following a coronary vascular distribution. Right, Precontrast T2‐weighted image of the same slice location as the image in the left panel. There is an increase in signal in the septum at the same area were the LGE was present.
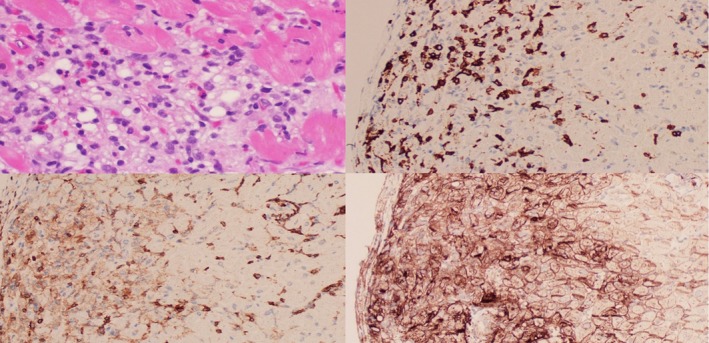
Pathological characteristics of immune checkpoint inhibitor–associated myocarditis. Top left, Hematoxylin and eosin stain of lymphocytic infiltration of myocarditis. Top right, Cluster of differentiation 8+ (CD8+) T‐cell immunohistochemical staining. Bottom left, CD4+ T‐cell immunohistochemical staining. Bottom right, Programmed death‐ligand 1+ immunohistochemical staining.
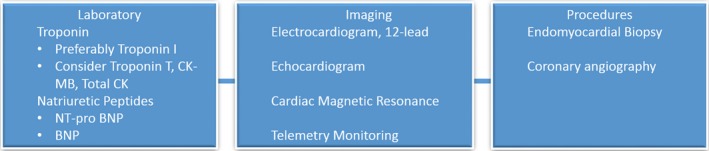
Diagnostic workup of suspected myocarditis. BNP indicates B‐type natriuretic peptide; CK, creatine kinase; CK‐MB, CK muscle/brain; NT‐proBNP, N‐terminal pro‐BNP.
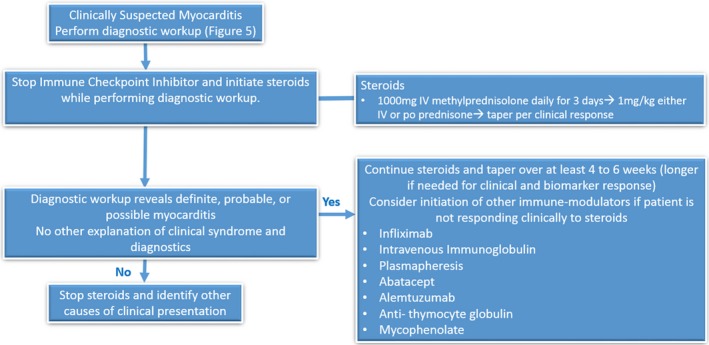
Treatment algorithm for suspected immune checkpoint inhibitor myocarditis.
References
-
- Wang DY, Salem J‐E, Cohen JV, Chandra S, Menzer C, Ye F, Zhao S, Das S, Beckermann KE, Ha L, Rathmell WK, Ancell KK, Balko JM, Bowman C, Davis EJ, Chism DD, Horn L, Long GV, Carlino MS, Lebrun‐Vignes B, Eroglu Z, Hassel JC, Menzies AM, Sosman JA, Sullivan RJ, Moslehi JJ, Johnson DB. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta‐analysis. JAMA Oncol. 2018;4:1721–1728. - PMC - PubMed
-
- Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, Hicks M, Puzanov I, Alexander MR, Bloomer TL, Becker JR, Slosky DA, Phillips EJ, Pilkinton MA, Craig‐Owens L, Kola N, Plautz G, Reshef DS, Deutsch JS, Deering RP, Olenchock BA, Lichtman AH, Roden DM, Seidman CE, Koralnik IJ, Seidman JG, Hoffman RD, Taube JM, Diaz LA Jr, Anders RA, Sosman JA, Moslehi JJ. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. 2016;375:1749–1755. - PMC - PubMed
-
- Mahmood SS, Fradley MG, Cohen JV, Nohria A, Reynolds KL, Heinzerling LM, Sullivan RJ, Damrongwatanasuk R, Chen CL, Gupta D, Kirchberger MC, Awadalla M, Hassan MZO, Moslehi JJ, Shah SP, Ganatra S, Thavendiranathan P, Lawrence DP, Groarke JD, Neilan TG. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. 2018;71:1755–1764. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
