

Prevalence and genetic profiles of isoniazid resistance in tuberculosis patients: A multicountry analysis of cross-sectional data
- PMID: 31961877
- PMCID: PMC6974034
- DOI: 10.1371/journal.pmed.1003008
Prevalence and genetic profiles of isoniazid resistance in tuberculosis patients: A multicountry analysis of cross-sectional data
Abstract
Background: The surveillance of drug resistance among tuberculosis (TB) patients is central to combatting the global TB epidemic and preventing the spread of antimicrobial resistance. Isoniazid and rifampicin are two of the most powerful first-line anti-TB medicines, and resistance to either of them increases the risk of treatment failure, relapse, or acquisition of resistance to other drugs. The global prevalence of rifampicin resistance is well documented, occurring in 3.4% (95% CI 2.5%-4.4%) of new TB patients and 18% (95% CI 7.6%-31%) of previously treated TB patients in 2018, whereas the prevalence of isoniazid resistance at global and regional levels is less understood. In 2018, the World Health Organization (WHO) recommended a modified 6-month treatment regimen for people with isoniazid-resistant, rifampicin-susceptible TB (Hr-TB), which includes rifampicin, pyrazinamide, ethambutol, and levofloxacin. We estimated the global prevalence of Hr-TB among TB patients and investigated associated phenotypic and genotypic drug resistance patterns.
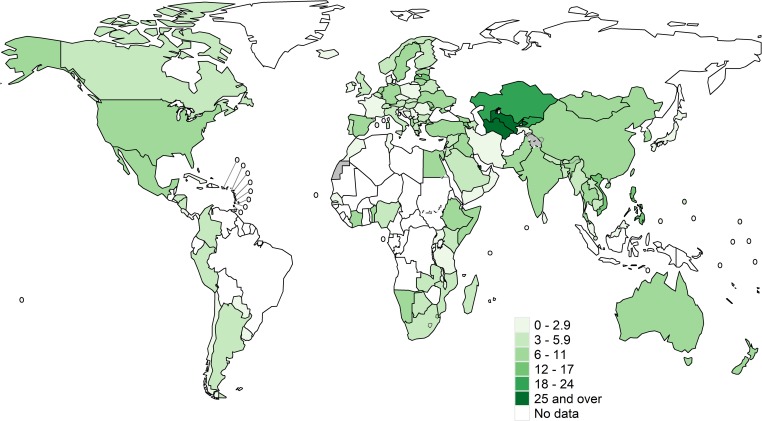
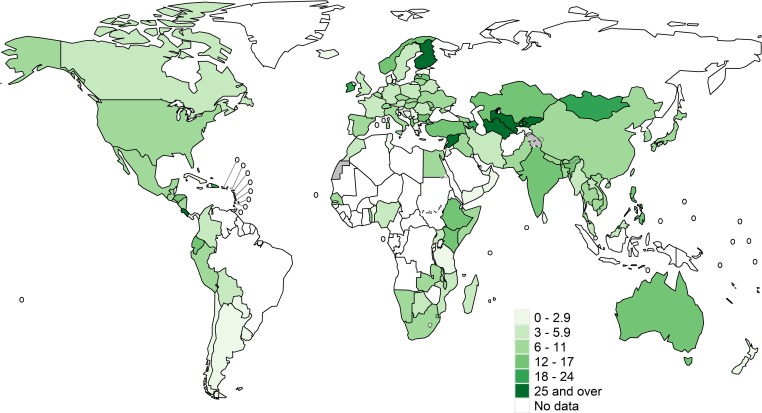
Methods and findings: Aggregated drug resistance data reported to WHO from either routine continuous surveillance or nationally representative periodic surveys of TB patients for the period 2003-2017 were reviewed. Isoniazid data were available from 156 countries or territories for 211,753 patients. Among these, the global prevalence of Hr-TB was 7.4% (95% CI 6.5%-8.4%) among new TB patients and 11.4% (95% CI 9.4%-13.4%) among previously treated TB patients. Additional data on pyrazinamide and levofloxacin resistance were available from 6 countries (Azerbaijan, Bangladesh, Belarus, Pakistan, the Philippines, and South Africa). There were no cases of resistance to both pyrazinamide and levofloxacin among Hr-TB patients, except for the Philippines (1.8%, 95% CI 0.2-6.4) and Belarus (5.3%, 95% CI 0.1-26.0). Sequencing data for all genomic regions involved in isoniazid resistance were available for 4,563 patients. Among the 1,174 isolates that were resistant by either phenotypic testing or sequencing, 78.6% (95% CI 76.1%-80.9%) had resistance-conferring mutations in the katG gene and 14.6% (95% CI 12.7%-16.8%) in both katG and the inhA promoter region. For 6.8% (95% CI 5.4%-8.4%) of patients, mutations occurred in the inhA promoter alone, for whom an increased dose of isoniazid may be considered. The main limitations of this study are that most analyses were performed at the national rather than individual patient level and that the quality of laboratory testing may vary between countries.
Conclusions: In this study, the prevalence of Hr-TB among TB patients was higher than the prevalence of rifampicin resistance globally. Many patients with Hr-TB would be missed by current diagnostic algorithms driven by rifampicin testing, highlighting the need for new rapid molecular technologies to ensure access to appropriate treatment and care. The low prevalence of resistance to pyrazinamide and fluoroquinolones among patients with Hr-TB provides further justification for the recommended modified treatment regimen.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: CUK is a consultant for the World Health Organization (WHO) Regional Office for Europe and QuantuMDx Group Ltd. CUK is an unpaid advisor to GenoScreen. CUK consulted for Becton Dickinson and the Foundation for Innovative New Diagnostics, which involved work for Cepheid Inc., Hain Lifescience, and WHO. The Bill & Melinda Gates Foundation, Janssen Pharmaceutica, and PerkinElmer covered CUK’s travel and accommodation to present at meetings. The Global Alliance for TB Drug Development Inc. and Otsuka Novel Products GmbH have supplied CUK with antibiotics for in vitro research. YD Diagnostics has provided assays for an evaluation by CUK. MCGA works with a government agency that provides technical advice to the National TB Control Program. Her agency also works closely with the Department of Health on matters of policy.
Figures
Comment in
-
Isoniazid-resistant tuberculosis: A problem we can no longer ignore.PLoS Med. 2020 Jan 21;17(1):e1003023. doi: 10.1371/journal.pmed.1003023. eCollection 2020 Jan. PLoS Med. 2020. PMID: 31961857 Free PMC article.
References
-
- World Health Organization. Global Tuberculosis Report. 2019.
-
- World Health Organization. WHO consolidated guidelines on drug-resistant tuberculosis treatment. 2019. - PubMed
-
- World Health Organization. Guidelines for treatment of drug-susceptible tuberculsois and patient care (2017 update). 2017. Available: http://www.who.int/tb/publications/2017/dstb_guidance_2017/en/
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
