

Different infusion durations for preventing platinum-induced hearing loss in children with cancer
- PMID: 31961948
- PMCID: PMC6984653
- DOI: 10.1002/14651858.CD010885.pub5
Different infusion durations for preventing platinum-induced hearing loss in children with cancer
Abstract
Background: Platinum-based therapy, including cisplatin, carboplatin or oxaliplatin, or a combination of these, is used to treat a variety of paediatric malignancies. Unfortunately, one of the most important adverse effects is the occurrence of hearing loss or ototoxicity. In an effort to prevent this ototoxicity, different platinum infusion durations have been studied. This review is the third update of a previously published Cochrane Review.
Objectives: To assess the effects of different durations of platinum infusion to prevent hearing loss or tinnitus, or both, in children with cancer. Secondary objectives were to assess possible effects of these infusion durations on: a) anti-tumour efficacy of platinum-based therapy, b) adverse effects other than hearing loss or tinnitus, and c) quality of life.
Search methods: We searched the electronic databases Cochrane Central Register of Controlled Trials (CENTRAL; the Cochrane Library 14 November 2019), MEDLINE (PubMed) (1945 to 14 November 2019) and Embase (Ovid) (1980 to 14 November 2019). In addition, we handsearched reference lists of relevant articles and we assessed the conference proceedings of the International Society for Paediatric Oncology (2009 up to and including 2019) and the American Society of Pediatric Hematology/Oncology (2014 up to and including 2019). We scanned ClinicalTrials.gov and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP; apps.who.int/trialsearch) for ongoing trials (both searched on 4 November 2019).
Selection criteria: Randomised controlled trials (RCTs) or controlled clinical trials (CCTs) comparing different platinum infusion durations in children with cancer. Only the platinum infusion duration could differ between the treatment groups.
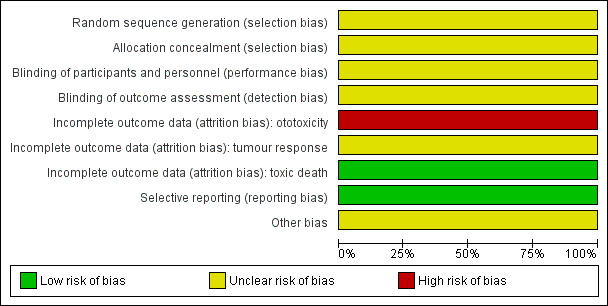
Data collection and analysis: Two review authors independently performed the study selection, 'Risk of bias' assessment and GRADE assessment of included studies, and data extraction including adverse effects. Analyses were performed according to the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions.
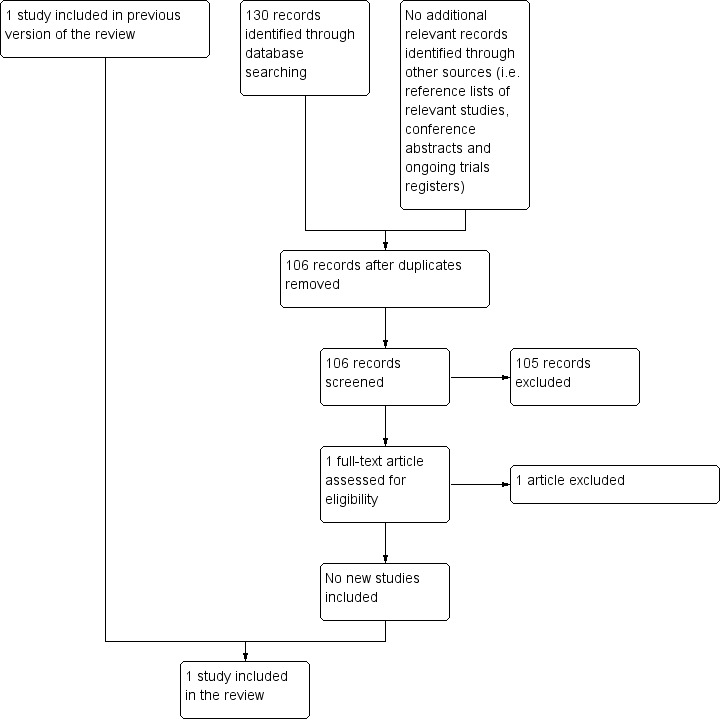
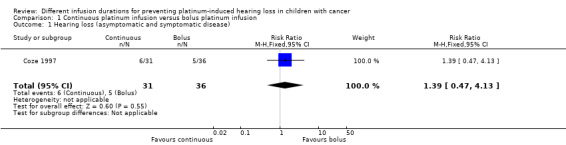
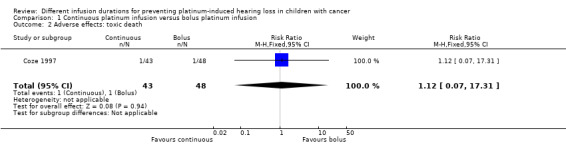
Main results: We identified one RCT and no CCTs; in this update no additional eligible studies were identified. The RCT (total number of children = 91) evaluated the use of a continuous cisplatin infusion (N = 43) versus a one-hour bolus cisplatin infusion (N = 48) in children with neuroblastoma. For the continuous infusion, cisplatin was administered on days one to five of the cycle, but it is unclear if the infusion duration was a total of five days. Risk of bias was present. Only results from shortly after induction therapy were provided. No clear evidence of a difference in hearing loss (defined as asymptomatic and symptomatic disease combined) between the different infusion durations was identified as results were imprecise (risk ratio (RR) 1.39, 95% confidence interval (CI) 0.47 to 4.13, low-quality evidence). Although the numbers of children were not provided, it was stated that tumour response was equivalent in both treatment arms. With regard to adverse effects other than ototoxicity, we were only able to assess toxic deaths. Again, the confidence interval of the estimated effect was too wide to exclude differences between the treatment groups (RR 1.12, 95% CI 0.07 to 17.31, low-quality evidence). No data were available for the other outcomes of interest (i.e. tinnitus, overall survival, event-free survival and quality of life) or for other (combinations of) infusion durations or other platinum analogues.
Authors' conclusions: Since only one eligible RCT evaluating the use of a continuous cisplatin infusion versus a one-hour bolus cisplatin infusion was found, and that had methodological limitations, no definitive conclusions can be made. It should be noted that 'no evidence of effect', as identified in this review, is not the same as 'evidence of no effect'. For other (combinations of) infusion durations and other platinum analogues no eligible studies were identified. More high-quality research is needed.
Copyright © 2020 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Conflict of interest statement
None known.
Figures


Update of
-
Different infusion durations for preventing platinum-induced hearing loss in children with cancer.Cochrane Database Syst Rev. 2018 Jul 5;7(7):CD010885. doi: 10.1002/14651858.CD010885.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2020 Jan 21;1:CD010885. doi: 10.1002/14651858.CD010885.pub5. PMID: 29975402 Free PMC article. Updated.
References
References to studies included in this review
Coze 1997 {published data only}
-
- Coze C, Hartmann O, Michon J, Frappaz D, Dusol F, Rubie H, et al. NB87 induction protocol for stage 4 neuroblastoma in children over 1 year of age: a report from the French Society of Pediatric Oncology. Journal of Clinical Oncology 1997;15(12):3433‐40. - PubMed
References to studies excluded from this review
Bergeron 2005 {published data only}
-
- Bergeron C, Dubourg L, Chastagner P, Mechinaud F, Plouvier E, Desfachelles AS, et al. Long‐term renal and hearing toxicity of carboplatin in infants treated for localized and unresectable neuroblastoma: results of the SFOP NBL90 study. Pediatric Blood & Cancer 2005;45(1):32‐6. - PubMed
Biswar 2017 {published data only}
-
- Biswas B, Ganguly S, Ghosh J, Batra A. Cisplatin‐induced hearing loss in children with cancer. The National Medical Journal of India 2017;30:327‐8. - PubMed
Lanvers‐Kaminsky 2006 {published data only}
-
- Lanvers‐Kaminsky C, Krefeld B, Dinnesen AG, Deuster D, Seifert E, Würthwein G, et al. Continuous or repeated prolonged cisplatin infusions in children: a prospective study on ototoxicity, platinum concentrations, and standard serum parameters. Pediatric Blood & Cancer 2006;47(2):183‐93. - PubMed
Additional references
Bertolini 2004
-
- Bertolini P, Lassalle M, Mercier G, Raquin MA, Izzi G, Corradini N, et al. Platinum compound‐related ototoxicity in children: long‐term follow‐up reveals continuous worsening of hearing loss. Journal of Pediatric Hematology/Oncology 2004;26(10):649‐55. - PubMed
Brock 1987
-
- Brock P, Yoeman L, Bellman S, Pritchard J. Ototoxicity in children treated with cis‐platinum (CDDP) for germ cell (GCT) and other tumours. Medical and Pediatric Oncology. 1987; Vol. 15:329 (abstract 138).
Brock 1991
-
- Brock PR, Bellman SC, Yeomans EC, Pinkerton CR, Pritchard J. Cisplatin ototoxicity in children: a practical grading system. Medical and Pediatric Oncology 1991;19(4):295‐300. - PubMed
Dean 2008
-
- Dean JB, Hayashi SS, Albert CM, King AA, Karzon R, Hayashi RJ. Hearing loss in pediatric oncology patients receiving carboplatin‐containing regimens. Journal of Pediatric Hematology/Oncology 2008;30(2):130‐4. - PubMed
Eloxatin SPC
-
- Eloxatin Summary of Product Characteristics. www.sanofi‐aventis.co.uk/products/Eloxatin_SPC.pdf (Accessed 2 March 2010).
Gallagher 1979
-
- Gallagher KL, Jones JK. Furosemide‐induced ototoxicity. Annals of Internal Medicine 1979;91(1):744‐5. - PubMed
Gietema 2000
-
- Gietema JA, Meinardi MT, Messerschmidt J, Gelevert T, Alt F, Uges DR, et al. Circulating plasma platinum more than 10 years after cisplatin treatment for testicular cancer. Lancet 2000;355(9209):1075‐6. - PubMed
GRADEpro GDT [Computer program]
-
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version 3.6.1. Hamilton (ON): McMaster University (developed by Evidence Prime), 2011.
Gregg 2004
-
- Gregg RB, Wiorek LS, Arvedson JC. Pediatric audiology: a review. Pediatrics in Review 2004;25(7):224‐33. - PubMed
Grewal 2010
Higgins 2011
-
- Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jenney 2005
-
- Jenney ME. Late effects of cancer treatment and current protective measures. In: Voûte PA, Barett A, Stevens MCG, Caron HN editor(s). Cancer in Children. 5th Edition. New York: Oxford University Press, 2005:123‐37.
Knight 2005
-
- Knight KR, Kraemer DF, Neuwelt EA. Ototoxicity in children receiving platinum chemotherapy: underestimating a commonly occurring toxicity that may influence academic and social development. Journal of Clinical Oncology 2005;23(34):8588‐96. - PubMed
Kremer 2016
-
- Kremer LC, Jellema P, Leclercq E, Noorman JK, Dalen EC. Cochrane Childhood Cancer Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)) 2016, Issue 5. Art. No.: CHILDCA.
Langer 2013
-
- Langer T, am Zehnhoff‐Dinnesen A, Radtke S, Meitert J, Zolk O. Understanding platinum‐induced ototoxicity. Trends in Pharmacological Sciences 2013;34(8):458‐69. - PubMed
Leahey 2012
-
- Leahey A. A cautionary tale: dosing chemotherapy in infants with retinoblastoma. Journal of Clinical Oncology 2012;30(10):1023‐4. - PubMed
Li 2004
-
- Li Y, Womer RB, Silber JH. Predicting cisplatin ototoxicity in children: the influence of age and the cumulative dose. European Journal of Cancer 2004;40(16):2445‐51. - PubMed
McHaney 1983
-
- McHaney VA, Thibadoux G, Hayes FA, Green AA. Hearing loss in children receiving cisplatin chemotherapy. Journal of Pediatrics 1983;102(2):314‐7. - PubMed
Meyer 2009
-
- Meyer AK, Young NM. Auditory late effects of chemotherapy. Cancer Treatment and Research 2009;150:195‐213. - PubMed
Qaddoumi 2012
Reddel 1982
-
- Reddel RR, Kefford RF, Grant JM, Coates AS, Fox RM, Tattersall MH. Ototoxicity in patients receiving cisplatin: importance of dose and method of drug administration. Cancer Treatment Reports 1982;66(1):19‐23. - PubMed
RevMan 2014 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Ross 2009
-
- Ross CJ, Katzov‐Eckert H, Dubé MP, Brooks B, Rassekh SR, Barhdadi A, et al. Genetic variants in TPMT and COMT are associated with hearing loss in children receiving cisplatin chemotherapy. Nature Genetics 2009;41(12):1345‐9. - PubMed
Schell 1989
-
- Schell MJ, McHaney VA, Green AA, Kun LE, Hayes FA, Horowitz M, et al. Hearing loss in children and young adults receiving cisplatin with or without prior cranial irradiation. Journal of Clinical Oncology 1989;7(6):754‐60. - PubMed
Skinner 2004
-
- Skinner R. Best practice in assessing ototoxicity in children with cancer. European Journal of Cancer 2004;40(16):2352‐4. - PubMed
Van As 2012
Van As 2014a
Van As 2016a
Van As 2016b
Van As 2019
Veal 2001
-
- Veal GJ, Dias C, Price L, Parry A, Errington J, Hale J, et al. Influence of cellular factors and pharmacokinetics on the formation of platinum‐DNA adducts in leukocytes of children receiving cisplatin therapy. Clinical Cancer Research 2001;7(8):2205‐12. - PubMed
WHO 1979
-
- World Health Organization. WHO Handbook for Reporting Results of Cancer Treatment. WHO offset publication no. 48. Geneva, Switzerland 1979.
References to other published versions of this review
Van As 2013
-
- As JW, Berg H, Dalen EC. Different infusion durations for preventing platinum‐induced hearing loss in children with cancer. Cochrane Database of Systematic Reviews 2013, Issue 12. [DOI: 10.1002/14651858.CD010885] - DOI
Van As 2014b
Van As 2016c
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources