

Dietary Folate Intake and Folic Acid Supplements among Pregnant Women from Southern Italy: Evidence from the "Mamma & Bambino" Cohort
- PMID: 31963813
- PMCID: PMC7013905
- DOI: 10.3390/ijerph17020638
Dietary Folate Intake and Folic Acid Supplements among Pregnant Women from Southern Italy: Evidence from the "Mamma & Bambino" Cohort
Abstract
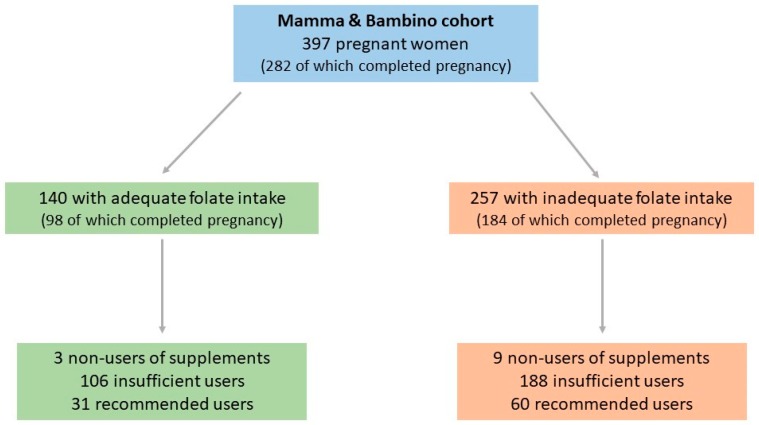
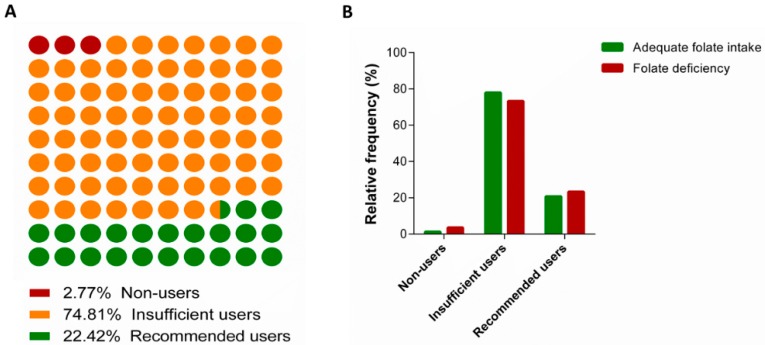
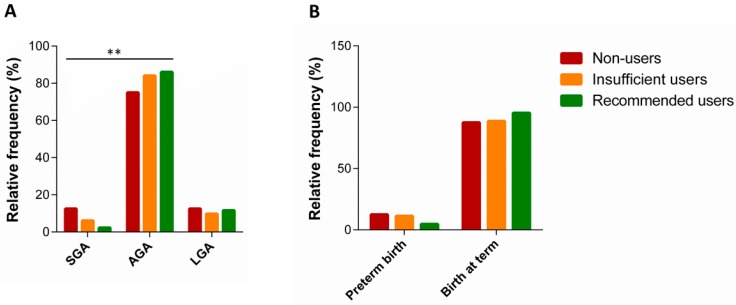
Folate requirement among women who plan to become pregnant should be raised to 600 μg/day during the periconceptional period. To meet this need, several countries began to promote the use of folic acid supplements before and during pregnancy. Here, we investigated prevalence and determinants of dietary folate intake and folic acid supplement use among 397 pregnant women (aged 15-50 years old, median = 37 years old). We also investigated their effects on neonatal outcomes in a subgroup of women who completed pregnancy. For doing that, we used data from the "Mamma & Bambino" project, an ongoing mother-child cohort settled in Catania (Italy). Inadequate folate intake was evaluated using a Food Frequency Questionnaire and defined as an intake < 600 μg/day. Women were also classified as non-users (i.e., women who did not use folic acid supplements), insufficient users (i.e., women who did not take folic acid supplements as recommended), and recommended users of folic acid supplements. Neonatal outcomes of interest were preterm birth (PTB) and small for gestational age (SGA). Nearly 65% of women (n = 257) reported inadequate folate intake, while 74.8% and 22.4% were respectively classified as insufficient or recommended users of supplements. We demonstrated higher odds of inadequate folate intake among smoking women (OR = 1.457; 95%CI = 1.046-2.030; p = 0.026), those who followed dietary restrictions (OR = 2.180; 95%CI = 1.085-4.378; p = 0.029), and those with low adherence to the Mediterranean Diet (OR = 3.194; 95%CI = 1.958-5.210; p < 0.001). In a subsample of 282 women who completed pregnancy, we also noted a higher percentage of SGA among those with inadequate folate intake (p < 0.001). Among 257 women with inadequate folate intake, those with low educational level were more likely to not take folic acid supplements than their more educated counterpart (OR = 5.574; 95%CI = 1.487-21.435; p = 0.012). In a subsample of 184 women with inadequate folate intake and complete pregnancy, we observed a higher proportion of SGA newborns among women who did not take supplement before pregnancy and those who did not take at all (p = 0.009). We also noted that the proportion of PTB was higher among non-users and insufficient users of folic acid supplements, but difference was not statistically significant. Our study underlined the need for improving the adherence of pregnant women with recommendations for dietary folate intake and supplement use. Although we proposed a protective effect of folic acid supplement use on risk of SGA, further research is encouraged to corroborate our findings and to investigate other factors involved.
Keywords: folate; neonatal outcomes; nutrition; pregnancy; public health.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bhutta Z.A., Das J.K., Rizvi A., Gaffey M.F., Walker N., Horton S., Webb P., Lartey A., Black R.E., Lancet Nutrition Interventions Review Group et al. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet. 2013;382:452–477. doi: 10.1016/S0140-6736(13)60996-4. - DOI - PubMed
-
- Black R.E., Victora C.G., Walker S.P., Bhutta Z.A., Christian P., De Onis M., Ezzati M., Grantham-McGregor S., Katz J., Martorell R., et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet. 2013;382:427–451. doi: 10.1016/S0140-6736(13)60937-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
