

Role for Maternal Asthma in Severe Human Metapneumovirus Lung Disease Susceptibility in Children
- PMID: 31965186
- PMCID: PMC7107446
- DOI: 10.1093/infdis/jiaa019
Role for Maternal Asthma in Severe Human Metapneumovirus Lung Disease Susceptibility in Children
Abstract
Background: Severity of human metapneumovirus (hMPV) lower respiratory illness (LRTI) is considered similar to that observed for respiratory syncytial virus (RSV). However, differences in severity between these pathogens have been noted, suggesting the degree of illness may vary in different populations. Moreover, a potential association between hMPV and asthma also suggests that hMPV may preferentially affect asthmatic subjects.
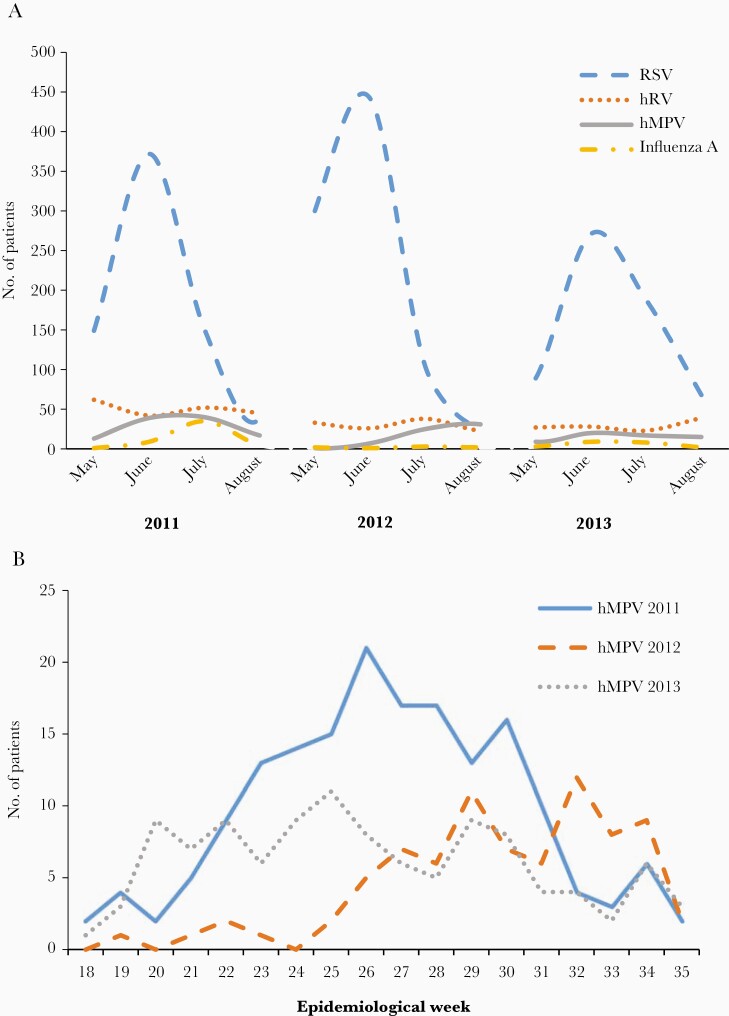
Methods: In a population-based surveillance study in children aged <2 years admitted for severe LRTI in Argentina, nasopharyngeal aspirates were tested by RT-PCR for hMPV, RSV, influenza A, and human rhinovirus.
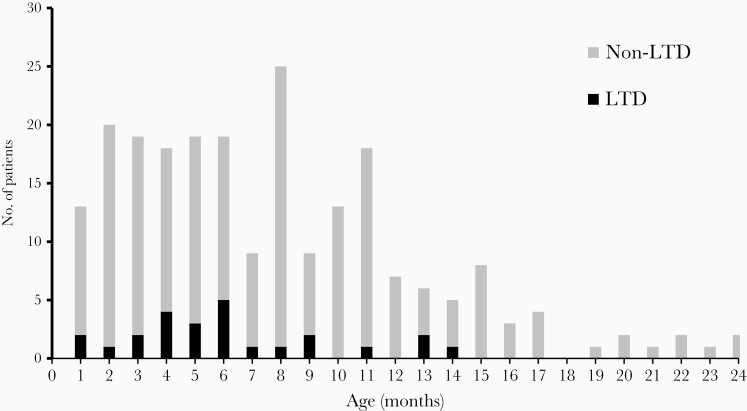
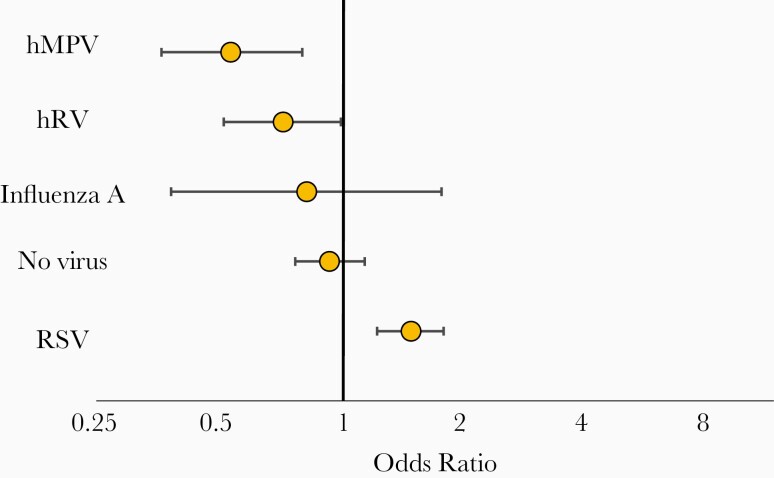
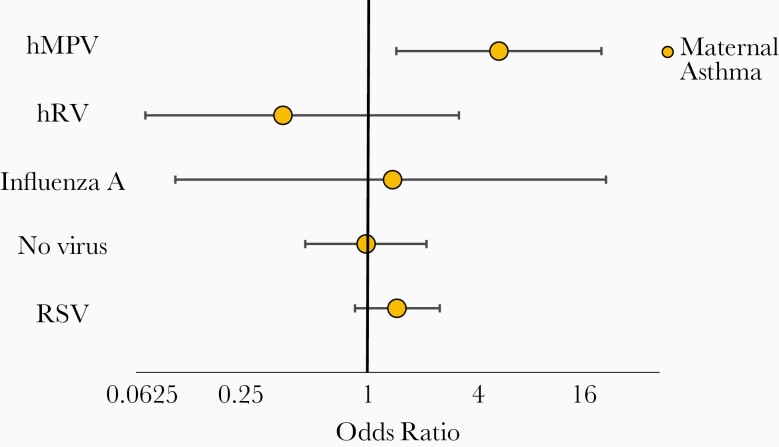
Results: Of 3947 children, 383 (10%) were infected with hMPV. The hospitalization rate for hMPV LRTI was 2.26 per 1000 children (95% confidence interval [CI], 2.04-2.49). Thirty-nine (10.2%) patients infected with hMPV experienced life-threatening disease (LTD; 0.23 per 1000 children; 95% CI, .16-.31/1000), and 2 died (mortality rate 0.024 per 1000; 95% CI, .003-.086). In hMPV-infected children birth to an asthmatic mother was an increased risk for LTD (odds ratio, 4.72; 95% CI, 1.39-16.01). We observed a specific interaction between maternal asthma and hMPV infection affecting risk for LTD.
Conclusions: Maternal asthma increases the risk for LTD in children <2 years old hospitalized for severe hMPV LRTI.
Keywords: burden of illness; children; human metapneumovirus; lower respiratory tract infection; maternal asthma; risk factors.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Nair H, Brooks WA, Katz M, et al. . Global burden of respiratory infections due to seasonal influenza in young children: a systematic review and meta-analysis. Lancet 2011; 378(9807):1917–30. - PubMed
-
- Anderson EJ, Simões EA, Buttery JP, et al. . Prevalence and characteristics of human metapneumovirus infection among hospitalized children at high risk for severe lower respiratory tract infection. J Pediatric Infect Dis Soc 2012; 1:212–22. - PubMed
-
- Laham FR, Israele V, Casellas JM, et al. . Differential production of inflammatory cytokines in primary infection with human metapneumovirus and with other common respiratory viruses of infancy. J Infect Dis 2004; 189:2047–56. - PubMed
