

Machine learning for the prediction of sepsis: a systematic review and meta-analysis of diagnostic test accuracy
- PMID: 31965266
- PMCID: PMC7067741
- DOI: 10.1007/s00134-019-05872-y
Machine learning for the prediction of sepsis: a systematic review and meta-analysis of diagnostic test accuracy
Abstract
Purpose: Early clinical recognition of sepsis can be challenging. With the advancement of machine learning, promising real-time models to predict sepsis have emerged. We assessed their performance by carrying out a systematic review and meta-analysis.
Methods: A systematic search was performed in PubMed, Embase.com and Scopus. Studies targeting sepsis, severe sepsis or septic shock in any hospital setting were eligible for inclusion. The index test was any supervised machine learning model for real-time prediction of these conditions. Quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology, with a tailored Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) checklist to evaluate risk of bias. Models with a reported area under the curve of the receiver operating characteristic (AUROC) metric were meta-analyzed to identify strongest contributors to model performance.
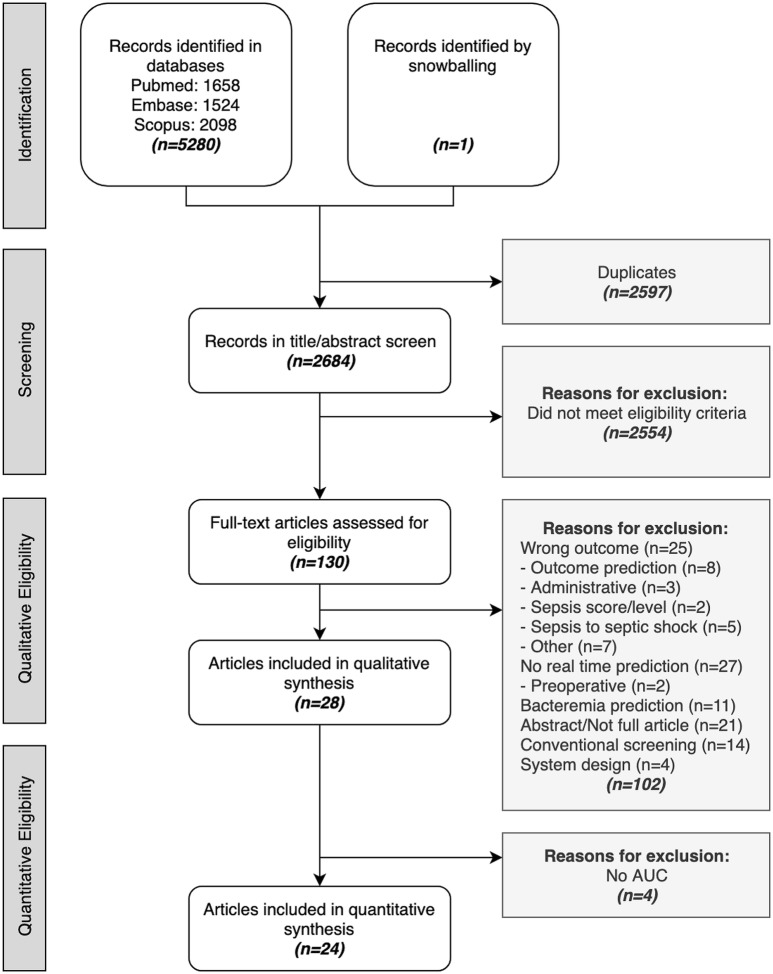
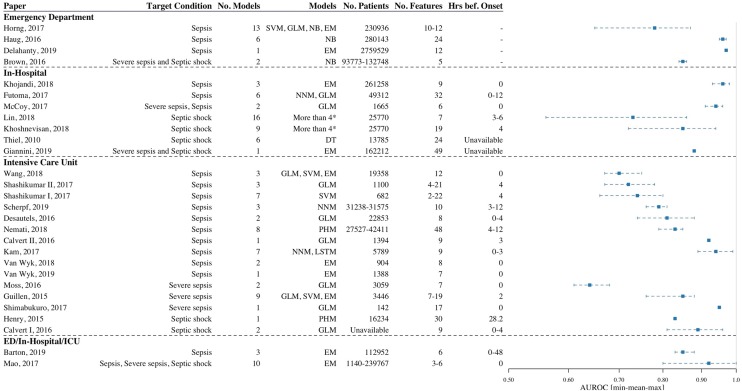
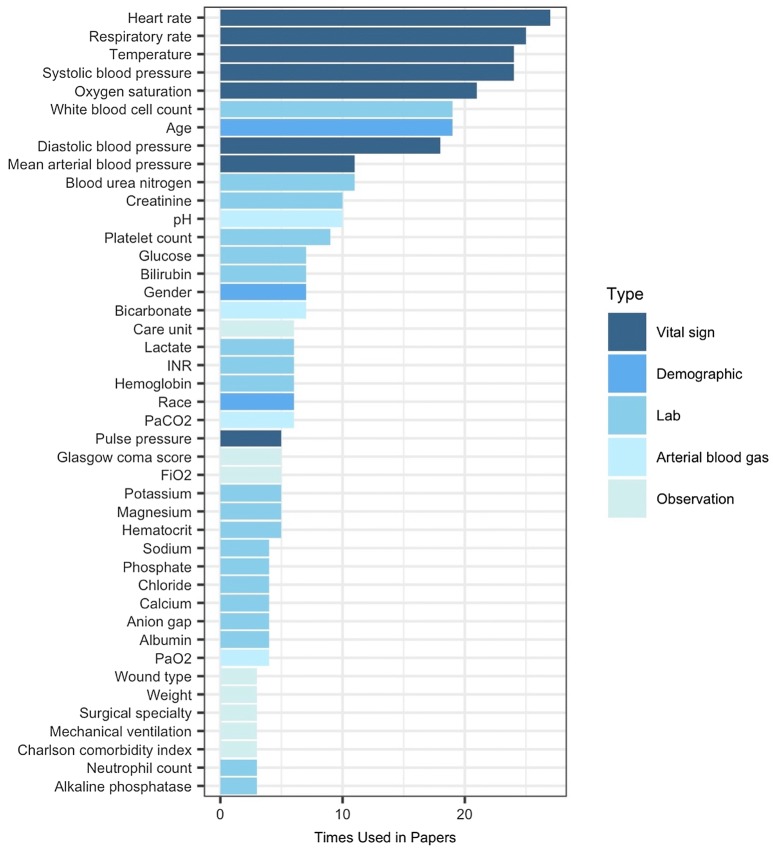
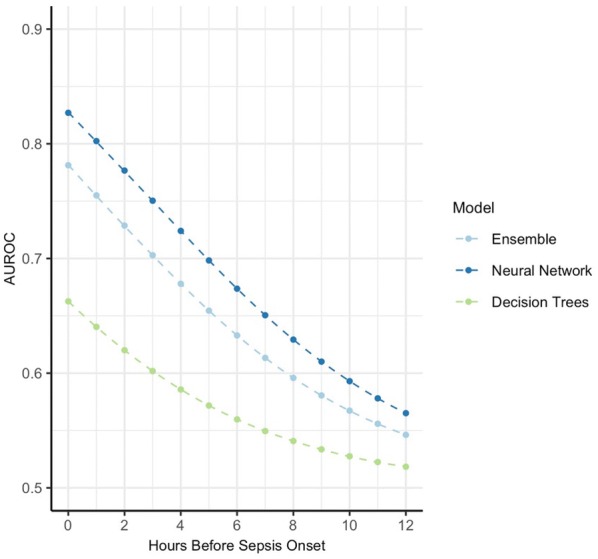
Results: After screening, a total of 28 papers were eligible for synthesis, from which 130 models were extracted. The majority of papers were developed in the intensive care unit (ICU, n = 15; 54%), followed by hospital wards (n = 7; 25%), the emergency department (ED, n = 4; 14%) and all of these settings (n = 2; 7%). For the prediction of sepsis, diagnostic test accuracy assessed by the AUROC ranged from 0.68-0.99 in the ICU, to 0.96-0.98 in-hospital and 0.87 to 0.97 in the ED. Varying sepsis definitions limit pooling of the performance across studies. Only three papers clinically implemented models with mixed results. In the multivariate analysis, temperature, lab values, and model type contributed most to model performance.
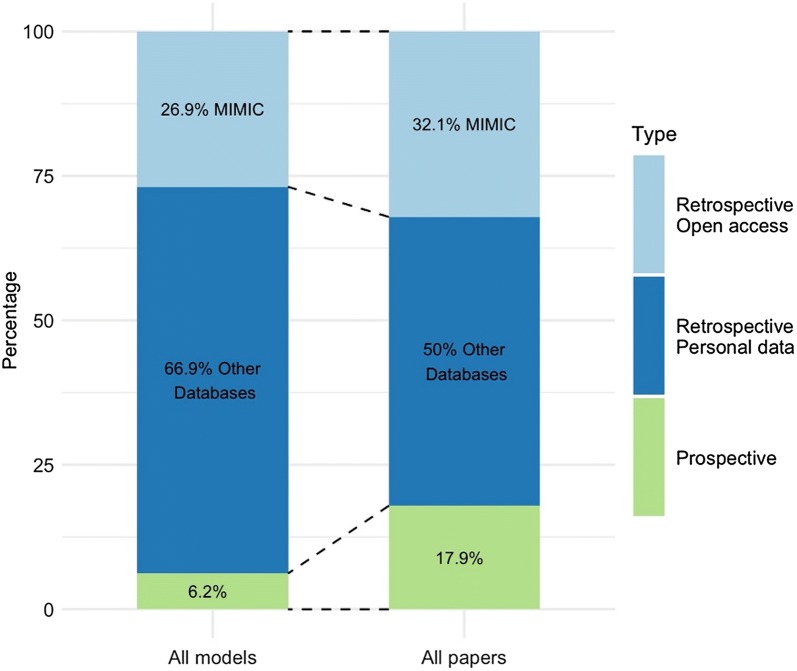
Conclusion: This systematic review and meta-analysis show that on retrospective data, individual machine learning models can accurately predict sepsis onset ahead of time. Although they present alternatives to traditional scoring systems, between-study heterogeneity limits the assessment of pooled results. Systematic reporting and clinical implementation studies are needed to bridge the gap between bytes and bedside.
Keywords: Machine learning; Meta-analysis; Prediction; Sepsis; Septic shock; Systematic review.
Conflict of interest statement
The author(s) declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
