

Multicenter Validation of Association Between Decline in MRI-PDFF and Histologic Response in NASH
- PMID: 31965579
- PMCID: PMC8055244
- DOI: 10.1002/hep.31121
Multicenter Validation of Association Between Decline in MRI-PDFF and Histologic Response in NASH
Abstract
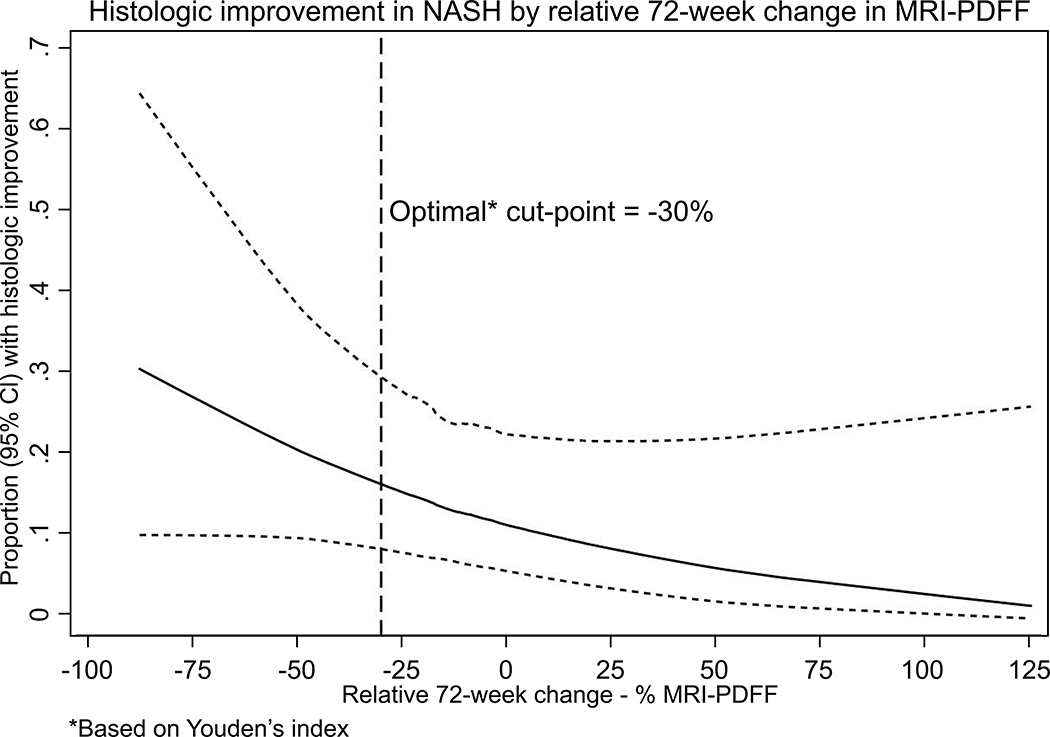
Background and aims: Emerging data from a single-center study suggests that a 30% relative reduction in liver fat content as assessed by magnetic resonance imaging-proton density fat fraction (MRI-PDFF) from baseline may be associated with histologic improvement in nonalcoholic steatohepatitis (NASH). There are limited multicenter data comparing an active drug versus placebo on the association between the quantity of liver fat reduction assessed by MRI-PDFF and histologic response in NASH. This study aims to examine the association between 30% relative reduction in MRI-PDFF and histologic response in obeticholic acid (OCA) versus placebo-treated patients in the FLINT (farnesoid X receptor ligand obeticholic acid in NASH trial).
Approach and results: This is a secondary analysis of the FLINT trial including 78 patients with MRI-PDFF measured before and after treatment along with paired liver histology assessment. Histologic response was defined as a 2-point improvement in nonalcoholic fatty liver disease activity score without worsening of fibrosis. OCA (25 mg orally once daily) was better than placebo in improving MRI-PDFF by an absolute difference of -3.4% (95% confidence interval [CI], -6.5 to -0.2%, P value = 0.04) and relative difference of -17% (95% CI, -34 to 0%, P value = 0.05). The optimal cutoff point for relative decline in MRI-PDFF for histologic response was 30% (using Youden's index). The rate of histologic response in those who achieved less than 30% decline in MRI-PDFF versus those who achieved a 30% or greater decline in MRI-PDFF (MRI-PDFF responders) relative to baseline was 19% versus 50%, respectively. Compared with MRI-PDFF nonresponders, MRI-PDFF responders demonstrated both a statistically and clinically significant higher odds 4.86 (95% CI, 1.4-12.8, P value < 0.009) of histologic response, including significant improvements in both steatosis and ballooning.
Conclusion: OCA was better than placebo in reducing liver fat. This multicenter trial provides data regarding the association between 30% decline in MRI-PDFF relative to baseline and histologic response in NASH.
Trial registration: ClinicalTrials.gov NCT01265498.
© 2020 by the American Association for the Study of Liver Diseases.
Figures
References
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67:328–357. - PubMed
-
- Williams CD, Stengel J, Asike MI, et al. Prevalence of nonalcoholic fatty liver disease and nonalcoholic steatohepatitis among a largely middle-aged population utilizing ultrasound and liver biopsy: a prospective study. Gastroenterology 2011;140:124–31. - PubMed
-
- Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med 2010;363:1341–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01DK061734/DK/NIDDK NIH HHS/United States
- UL1TR000058/TR/NCATS NIH HHS/United States
- UL1TR000439/TR/NCATS NIH HHS/United States
- UL1 TR000006/TR/NCATS NIH HHS/United States
- UL1 TR000058/TR/NCATS NIH HHS/United States
- U01 DK061728/DK/NIDDK NIH HHS/United States
- UL1TR000423/TR/NCATS NIH HHS/United States
- R01 DK106419/DK/NIDDK NIH HHS/United States
- UL1 TR003098/TR/NCATS NIH HHS/United States
- U01 DK061737/DK/NIDDK NIH HHS/United States
- U01 DK061713/DK/NIDDK NIH HHS/United States
- UL1 TR002649/TR/NCATS NIH HHS/United States
- U01DK061731/DK/NIDDK NIH HHS/United States
- U01 DK061732/DK/NIDDK NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- UL1TR000454/TR/NCATS NIH HHS/United States
- U01 DK061731/DK/NIDDK NIH HHS/United States
- U01 DK061718/DK/NIDDK NIH HHS/United States
- UL1 TR001442/TR/NCATS NIH HHS/United States
- P30 DK120515/DK/NIDDK NIH HHS/United States
- UL1TR000150/TR/NCATS NIH HHS/United States
- U01DK061738/DK/NIDDK NIH HHS/United States
- UL1 TR000436/TR/NCATS NIH HHS/United States
- UL1TR000077/TR/NCATS NIH HHS/United States
- U01DK061728/DK/NIDDK NIH HHS/United States
- U01 DK061730/DK/NIDDK NIH HHS/United States
- U24 DK061730/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UL1TR000424/TR/NCATS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- R01DK106419/DK/NIDDK NIH HHS/United States
- U01 DK061738/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- U01DK061730/DK/NIDDK NIH HHS/United States
- U01DK061737/DK/NIDDK NIH HHS/United States
- U01DK061718/DK/NIDDK NIH HHS/United States
- P30DK120515/DK/NIDDK NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- U01 DK061734/DK/NIDDK NIH HHS/United States
- UL1TR000004/TR/NCATS NIH HHS/United States
- U01DK061713/DK/NIDDK NIH HHS/United States
- UL1TR000040/TR/NCATS NIH HHS/United States
- UL1TR000436/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
- U01DK061732/DK/NIDDK NIH HHS/United States
- UL1 TR000423/TR/NCATS NIH HHS/United States
- UL1 TR000100/TR/NCATS NIH HHS/United States
- UL1TR000006/TR/NCATS NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- UL1 TR002345/TR/NCATS NIH HHS/United States
- UL1TR000448/TR/NCATS NIH HHS/United States
- UL1TR000100/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
