

Early diagnosis of sepsis in emergency departments, time to treatment, and association with mortality: An observational study
- PMID: 31968009
- PMCID: PMC6975530
- DOI: 10.1371/journal.pone.0227652
Early diagnosis of sepsis in emergency departments, time to treatment, and association with mortality: An observational study
Erratum in
-
Correction: Early diagnosis of sepsis in emergency departments, time to treatment, and association with mortality: An observational study.PLoS One. 2021 Mar 15;16(3):e0248879. doi: 10.1371/journal.pone.0248879. eCollection 2021. PLoS One. 2021. PMID: 33720978 Free PMC article.
Abstract
Background: Early recognition of sepsis is critical for timely initiation of treatment. The first objective of this study was to assess the timeliness of diagnostic procedures for recognizing sepsis in emergency departments. We define diagnostic procedures as tests used to help diagnose the condition of patients. The second objective was to estimate associations between diagnostic procedures and time to antibiotic treatment, and to estimate associations between time to antibiotic treatment and mortality.
Methods: This observational study from 24 emergency departments in Norway included 1559 patients with infection and at least two systemic inflammatory response syndrome criteria. We estimated associations using linear and logistic regression analyses.
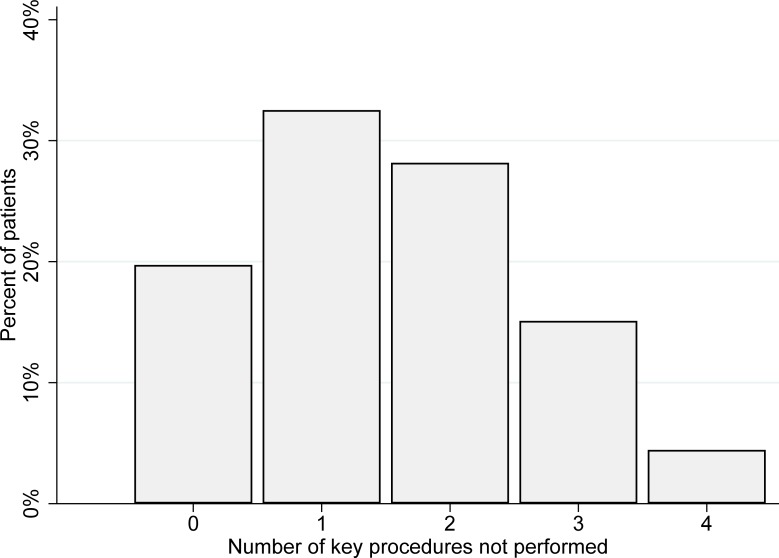
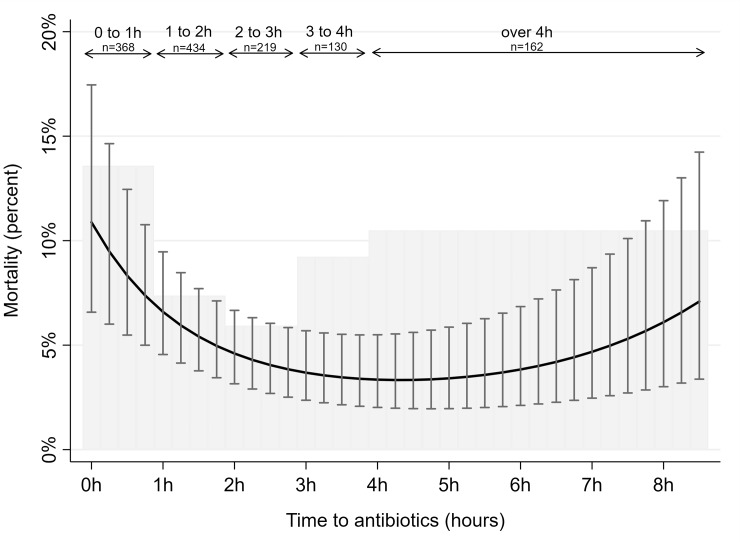
Results: Of the study patients, 72.9% (CI 70.7-75.1) had documented triage within 15 minutes of presentation to the emergency departments, 44.9% (42.4-47.4) were examined by a physician in accordance with the triage priority, 44.4% (41.4-46.9) were adequately observed through continual monitoring of signs while in the emergency department, and 25.4% (23.2-27.7) received antibiotics within 1 hour. Delay or non-completion of these key diagnostic procedures predicted a delay of more than 2.5 hours to antibiotic treatment. Patients who received antibiotics within 1 hour had an observed 30-day all-cause mortality of 13.6% (10.1-17.1), in the timespan 2 to 3 hours after admission 5.9% (2.8-9.1), and 4 hours or later after admission 10.5% (5.7-15.3).
Conclusions: Key procedures for recognizing sepsis were delayed or not completed in a substantial proportion of patients admitted to the emergency department with sepsis. Delay or non-completion of key diagnostic procedures was associated with prolonged time to treatment with antibiotics. This suggests a need for systematic improvement in the initial management of patients admitted to emergency departments with sepsis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
