

Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer: A Randomized Clinical Trial
- PMID: 31968063
- PMCID: PMC6990653
- DOI: 10.1001/jamasurg.2019.5474
Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer: A Randomized Clinical Trial
Erratum in
-
Error in Affiliations.JAMA Surg. 2020 Mar 1;155(3):269. doi: 10.1001/jamasurg.2020.0188. JAMA Surg. 2020. PMID: 32186696 Free PMC article. No abstract available.
Abstract
Importance: Research supports use of prehabilitation to optimize physical status before and after colorectal cancer resection, but its effect on postoperative complications remains unclear. Frail patients are a target for prehabilitation interventions owing to increased risk for poor postoperative outcomes.
Objective: To assess the extent to which a prehabilitation program affects 30-day postoperative complications in frail patients undergoing colorectal cancer resection compared with postoperative rehabilitation.
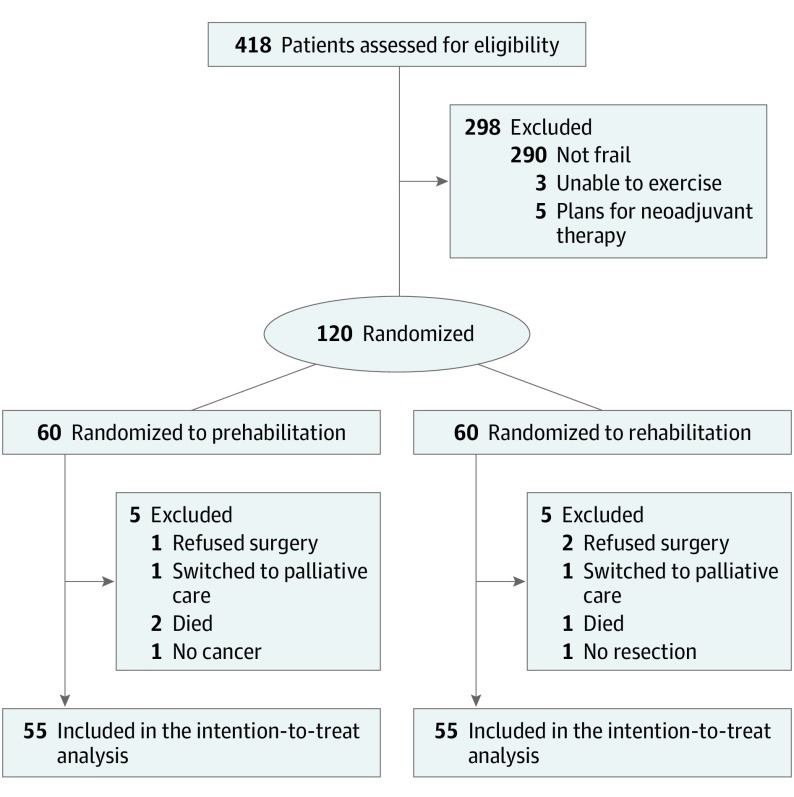
Design, setting, and participants: This single-blind, parallel-arm, superiority randomized clinical trial recruited patients undergoing colorectal cancer resection from September 7, 2015, through June 19, 2019. Patients were followed up for 4 weeks before surgery and 4 weeks after surgery at 2 university-affiliated tertiary hospitals. A total of 418 patients 65 years or older were assessed for eligibility. Of these, 298 patients were excluded (not frail [n = 290], unable to exercise [n = 3], and planned neoadjuvant treatment [n = 5]), and 120 frail patients (Fried Frailty Index,≥2) were randomized. Ten patients were excluded after randomization because they refused surgery (n = 3), died before surgery (n = 3), had no cancer (n = 1), had surgery without bowel resection (n = 1), or were switched to palliative care (n = 2). Hence, 110 patients were included in the intention-to-treat analysis (55 in the prehabilitation [Prehab] and 55 in the rehabilitation [Rehab] groups). Data were analyzed from July 25 through August 21, 2019.
Interventions: Multimodal program involving exercise, nutritional, and psychological interventions initiated before (Prehab group) or after (Rehab group) surgery. All patients were treated within a standardized enhanced recovery pathway.
Main outcomes and measures: The primary outcome included the Comprehensive Complications Index measured at 30 days after surgery. Secondary outcomes were 30-day overall and severe complications, primary and total length of hospital stay, 30-day emergency department visits and hospital readmissions, recovery of walking capacity, and patient-reported outcome measures.
Results: Of 110 patients randomized, mean (SD) age was 78 (7) years; 52 (47.3%) were men and 58 (52.7%) were women; 31 (28.2%) had rectal cancer; and 87 (79.1%) underwent minimally invasive surgery. There was no between-group difference in the primary outcome measure, 30-day Comprehensive Complications Index (adjusted mean difference, -3.2; 95% CI, -11.8 to 5.3; P = .45). Secondary outcome measures were also not different between groups.
Conclusions and relevance: In frail patients undergoing colorectal cancer resection (predominantly minimally invasive) within an enhanced recovery pathway, a multimodal prehabilitation program did not affect postoperative outcomes. Alternative strategies should be considered to optimize treatment of frail patients preoperatively.
Trial registration: ClinicalTrials.gov identifier: NCT02502760.
Conflict of interest statement
Comment in
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):896. doi: 10.1001/jamasurg.2020.1798. JAMA Surg. 2020. PMID: 32584923 No abstract available.
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):898-899. doi: 10.1001/jamasurg.2020.1813. JAMA Surg. 2020. PMID: 32584938 No abstract available.
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):899-900. doi: 10.1001/jamasurg.2020.1816. JAMA Surg. 2020. PMID: 32584941 No abstract available.
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):896-897. doi: 10.1001/jamasurg.2020.1801. JAMA Surg. 2020. PMID: 32584944 No abstract available.
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):897-898. doi: 10.1001/jamasurg.2020.1807. JAMA Surg. 2020. PMID: 32584947 No abstract available.
-
Prehabilitation vs Postoperative Rehabilitation for Frail Patients.JAMA Surg. 2020 Sep 1;155(9):897. doi: 10.1001/jamasurg.2020.1804. JAMA Surg. 2020. PMID: 32585010 No abstract available.
-
Re: Effect of Multimodal Prehabilitation vs Postoperative Rehabilitation on 30-Day Postoperative Complications for Frail Patients Undergoing Resection of Colorectal Cancer: A Randomized Clinical Trial.J Urol. 2020 Oct;204(4):869-870. doi: 10.1097/JU.0000000000001215.02. Epub 2020 Jul 23. J Urol. 2020. PMID: 32701372 No abstract available.
References
-
- Canadian Cancer Society Colorectal cancer statistics. https://www.cancer.ca/en/cancer-information/cancer-type/colorectal/stati.... 2015. Accessed March 4, 2015.
-
- Surveillance, Epidemiology, and End Results Program, National Cancer Institute Cancer Stat Facts: Colorectal Cancer. https://seer.cancer.gov/statfacts/html/colorect.html. 2015. Accessed March 4, 2015.
-
- National Cancer Registration and Analysis Service Cancer and equality groups: key metrics. http://www.ncin.org.uk/cancer_type_and_topic_specific_work/topic_specifi.... 2015. Accessed March 4, 2015.
