

A Phase II Basket Trial of Dual Anti-CTLA-4 and Anti-PD-1 Blockade in Rare Tumors (DART SWOG 1609) in Patients with Nonpancreatic Neuroendocrine Tumors
- PMID: 31969335
- PMCID: PMC7231627
- DOI: 10.1158/1078-0432.CCR-19-3356
A Phase II Basket Trial of Dual Anti-CTLA-4 and Anti-PD-1 Blockade in Rare Tumors (DART SWOG 1609) in Patients with Nonpancreatic Neuroendocrine Tumors
Abstract
Purpose: Immune checkpoint blockade has improved outcomes across tumor types; little is known about the efficacy of these agents in rare tumors. We report the results of the (nonpancreatic) neuroendocrine neoplasm cohort of SWOG S1609 dual anti-CTLA-4 and anti-PD-1 blockade in rare tumors (DART).
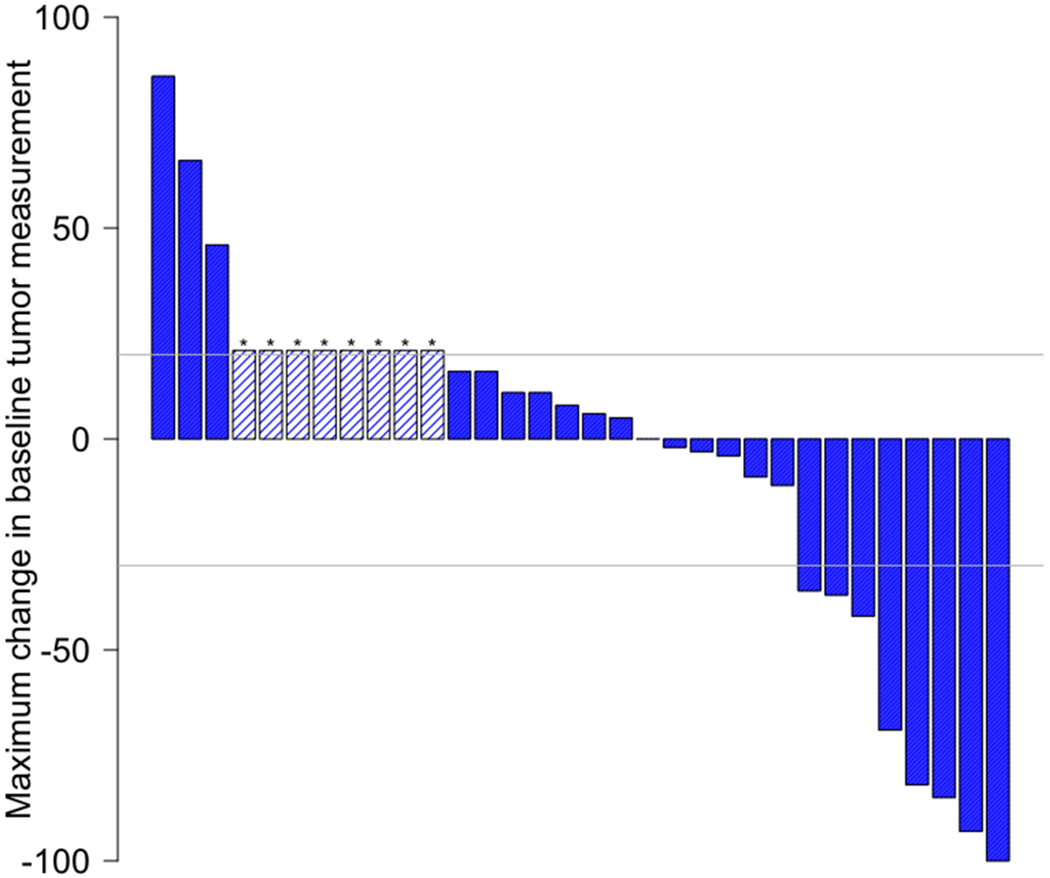
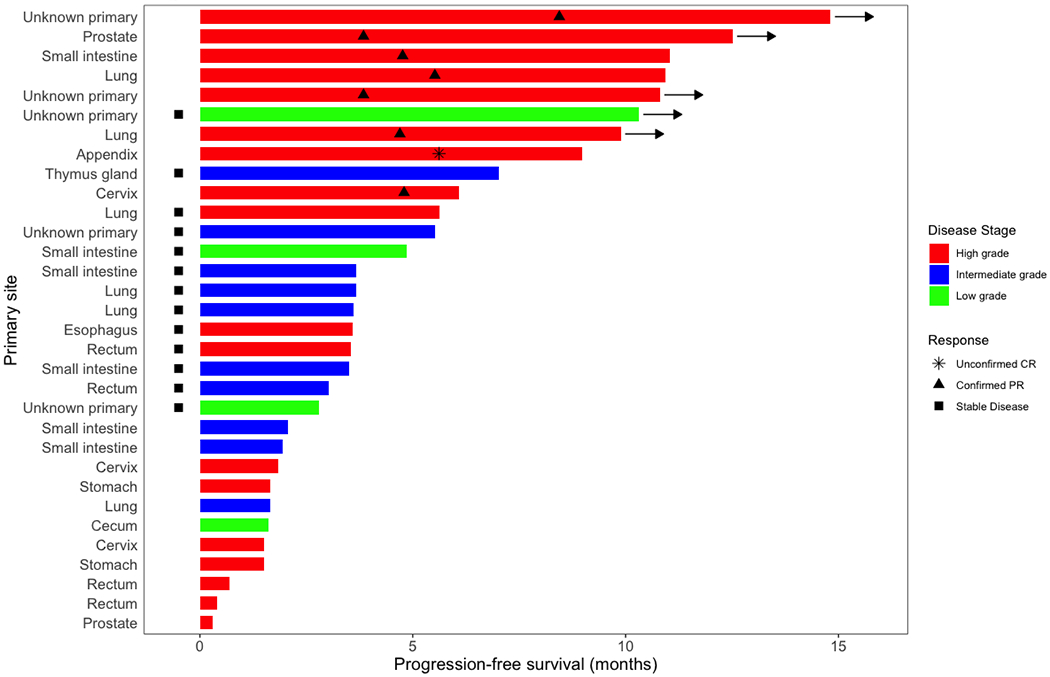
Patients and methods: We performed a prospective, open-label, multicenter phase II clinical trial of ipilimumab plus nivolumab across multiple rare tumor cohorts, with the (nonpancreatic) neuroendocrine cohort reported here. Response assessment by grade was not prespecified. The primary endpoint was overall response rate [ORR; RECIST v1.1; complete response (CR) and partial response (PR)]; secondary endpoints included progression-free survival (PFS), overall survival (OS), stable disease >6 months, and toxicity.
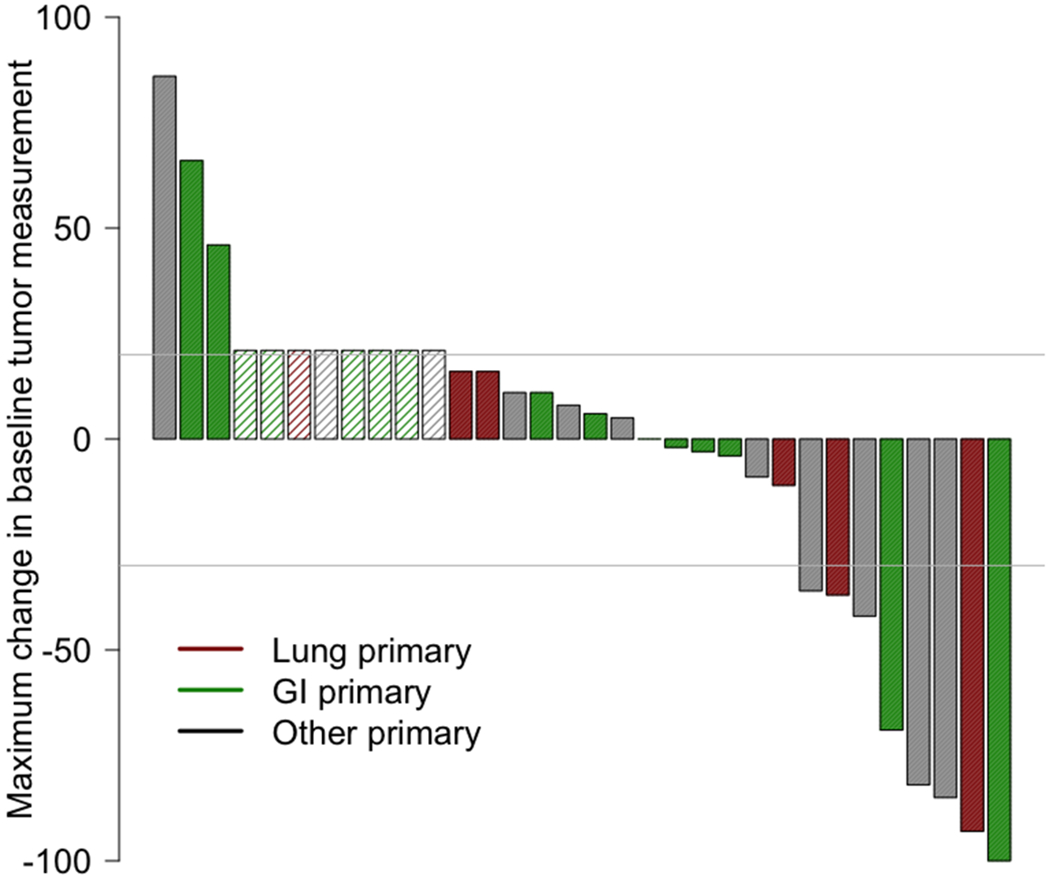
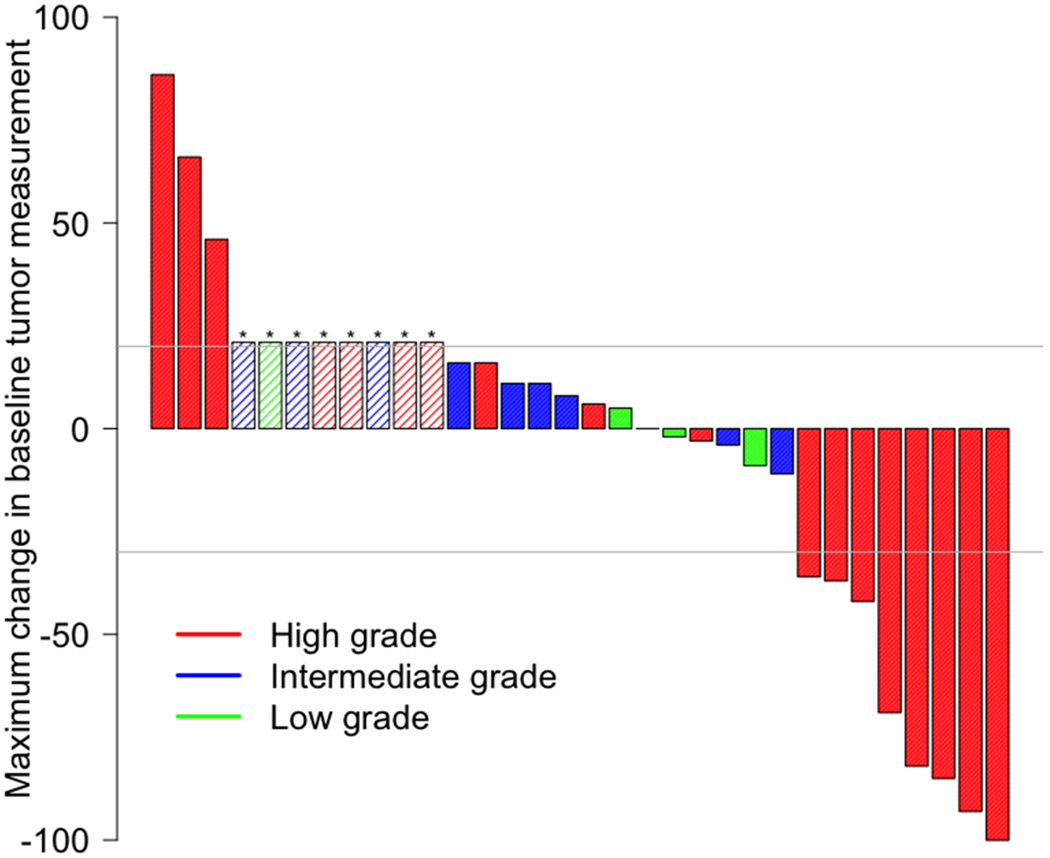
Results: Thirty-two eligible patients received therapy; 18 (56%) had high-grade disease. Most common primary sites were gastrointestinal (47%; N = 15) and lung (19%; N = 6). The overall ORR was 25% [95% confidence interval (CI) 13-64%; CR, 3%, N = 1; PR, 22%, N = 7]. Patients with high-grade neuroendocrine carcinoma had an ORR of 44% (8/18 patients) versus 0% in low/intermediate grade tumors (0/14 patients; P = 0.004). The 6-month PFS was 31% (95% CI, 19%-52%); median OS was 11 months (95% CI, 6-∞). The most common toxicities were hypothyroidism (31%), fatigue (28%), and nausea (28%), with alanine aminotransferase elevation (9%) as the most common grade 3/4 immune-related adverse event, and no grade 5 events.
Conclusions: Ipilimumab plus nivolumab demonstrated a 44% ORR in patients with nonpancreatic high-grade neuroendocrine carcinoma, with 0% ORR in low/intermediate grade disease.
Trial registration: ClinicalTrials.gov NCT02834013.
©2020 American Association for Cancer Research.
Figures
Comment in
-
Ipilimumab and Nivolumab in Rare Tumors S1609: Neuroendocrine-Letter.Clin Cancer Res. 2020 May 15;26(10):2433. doi: 10.1158/1078-0432.CCR-20-0443. Clin Cancer Res. 2020. PMID: 32414760 No abstract available.
-
Ipilimumab and Nivolumab in Rare Tumors S1609: Neuroendocrine-Response.Clin Cancer Res. 2020 May 15;26(10):2434. doi: 10.1158/1078-0432.CCR-20-0790. Clin Cancer Res. 2020. PMID: 32414761 No abstract available.
References
-
- Luo G, Javed A, Strosberg JR, Jin K, Zhang Y, Liu C, et al. Modified Staging Classification for Pancreatic Neuroendocrine Tumors on the Basis of the American Joint Committee on Cancer and European Neuroendocrine Tumor Society Systems. Journal of Clinical Oncology 2017;35(3):274–80 doi 10.1200/jco.2016.67.8193. - DOI - PubMed
-
- Brookmeyer R, Crowley J. A k-sample median test for censored data. Journal of the American Statistical Association 1982;77(378):433–40.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UG1 CA189873/CA/NCI NIH HHS/United States
- U10 CA180858/CA/NCI NIH HHS/United States
- UG1 CA233324/CA/NCI NIH HHS/United States
- U10 CA180850/CA/NCI NIH HHS/United States
- UG1 CA233160/CA/NCI NIH HHS/United States
- UG1 CA189830/CA/NCI NIH HHS/United States
- UG1 CA189809/CA/NCI NIH HHS/United States
- P30 CA023100/CA/NCI NIH HHS/United States
- U10 CA073590/CA/NCI NIH HHS/United States
- U10 CA180820/CA/NCI NIH HHS/United States
- U10 CA180888/CA/NCI NIH HHS/United States
- UG1 CA189856/CA/NCI NIH HHS/United States
- UG1 CA233331/CA/NCI NIH HHS/United States
- UG1 CA189971/CA/NCI NIH HHS/United States
- U10 CA012644/CA/NCI NIH HHS/United States
- U10 CA180834/CA/NCI NIH HHS/United States
- UG1 CA233329/CA/NCI NIH HHS/United States
- UG1 CA189821/CA/NCI NIH HHS/United States
- UG1 CA189870/CA/NCI NIH HHS/United States
- U10 CA180821/CA/NCI NIH HHS/United States
- U10 CA180801/CA/NCI NIH HHS/United States
- U10 CA180819/CA/NCI NIH HHS/United States
- UG1 CA189953/CA/NCI NIH HHS/United States
