Direct and indirect healthcare costs of lung cancer CT screening in Denmark: a registry study
- PMID: 31969362
- PMCID: PMC7045232
- DOI: 10.1136/bmjopen-2019-031768
Direct and indirect healthcare costs of lung cancer CT screening in Denmark: a registry study
Abstract
Introduction: A study based on the Danish Randomised Controlled Lung Cancer Screening Trial (DLCST) calculated the healthcare costs of lung cancer screening by comparing costs in an intervention group with a control group. Participants in both groups, however, experienced significantly increased negative psychosocial consequences after randomisation. Substantial participation bias has also been documented: The DLCST participants reported fewer negative psychosocial aspects and experienced better living conditions compared with the random sample.
Objective: To comprehensively analyse the costs of lung cancer CT screening and to determine whether invitations to mass screening alter the utilisation of the healthcare system resulting in indirect costs. Healthcare utilisation and costs are analysed in the primary care sector (general practitioner psychologists, physiotherapists, other specialists, drugs) and the secondary care sector (emergency room contacts, outpatient visits, hospitalisation days, surgical procedures and non-surgical procedures).
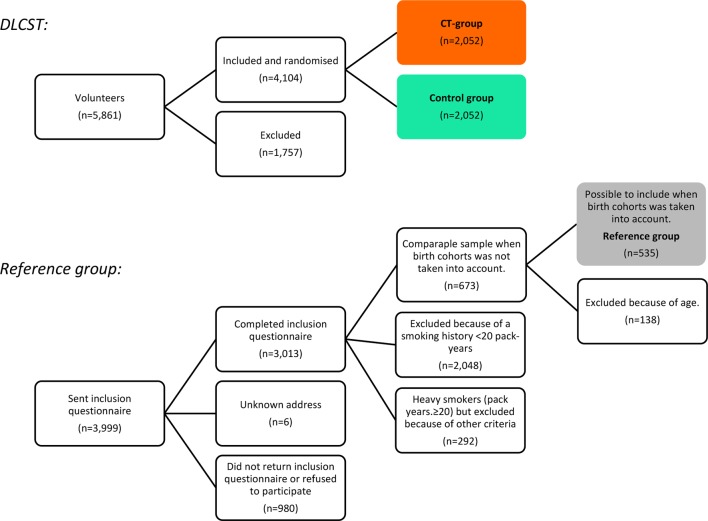
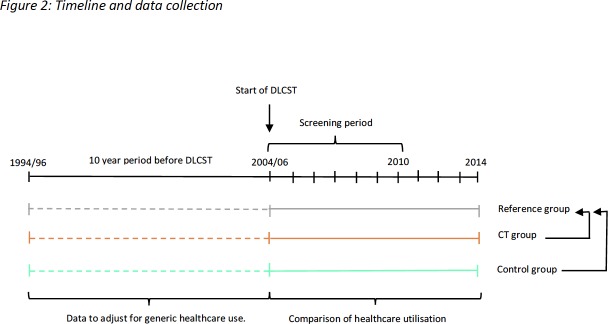
Design: To account for bias in the original trial, the costs and utilisation of healthcare by participants in DLCST were compared with a new reference group, selected in the period from randomisation (2004-2006) until 2014.
Setting: Four Danish national registers.
Participants: DLCST included 4104 current or former heavy smokers, randomly assigned to the CT group or the control group. The new reference group comprised a random sample of 535 current or former heavy smokers in the general Danish population who were never invited to participate in a cancer screening test.
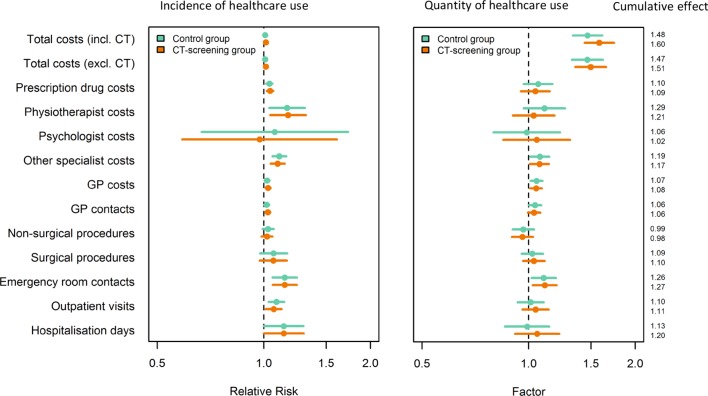
Main outcome measures: Total healthcare costs including costs and utilisation of healthcare in both the primary and the secondary care sector.
Results: Compared with the reference group, the participants in both the CT group (offered annual CT screening, lung function test and smoking counselling) and the control group (offered annual lung function test and smoking counselling) had significantly increased total healthcare costs, calculated at 60% and 48% respectively. The increase in costs was caused by increased use of healthcare in both the primary and the secondary sectors.
Conclusion: CT screening leads to 60% increased total healthcare costs. Such increase would raise the expected annual healthcare cost per participant from EUR 2348 to EUR 3756. Cost analysis that only includes costs directly related to the CT scan and follow-up procedures most likely underestimates total costs. Our data show that the increased costs are not limited to the secondary sector.
Trial registration number: NCT00496977.
Keywords: CT scan; cancer screening test; healthcare cost; illness perception; lung cancer; mass screening.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at ‘http://www.icmje.org/coi_disclosure.pdf’.
Figures