

Postoperative Horner's syndrome following excision of incidental cervical ganglioneuroma during hemithyroidectomy and parathyroid gland exploration
- PMID: 31969402
- PMCID: PMC7021161
- DOI: 10.1136/bcr-2019-231514
Postoperative Horner's syndrome following excision of incidental cervical ganglioneuroma during hemithyroidectomy and parathyroid gland exploration
Abstract
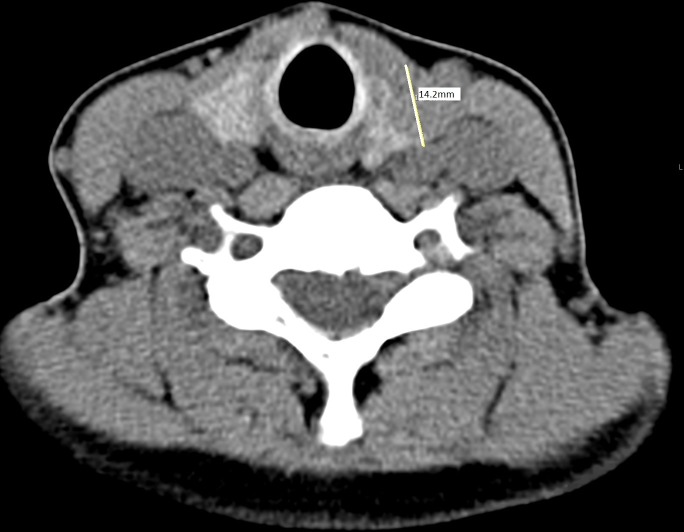
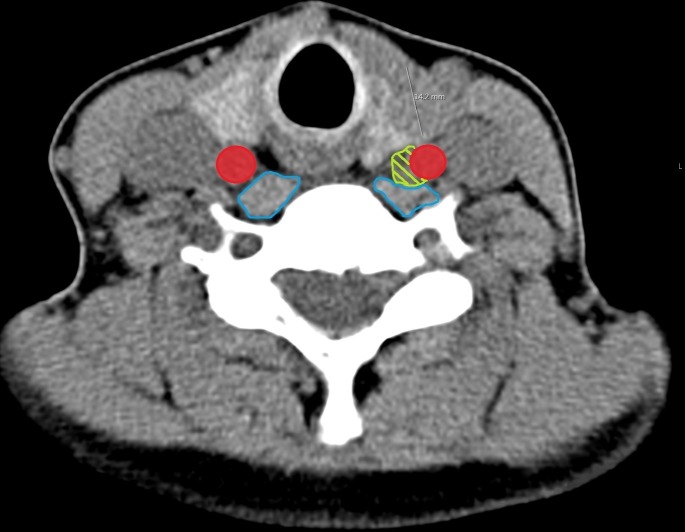
This 49-year-old woman was referred to ear, nose and throat (ENT) with primary hyperparathyroidism. Imaging studies failed to localise the adenoma so she required four-gland parathyroid exploration. She also required diagnostic left hemithyroidectomy as she had a U3 nodule with multiple insufficient fine needle aspirations (FNAs). Intraoperatively, the left thyroidectomy proceeded uneventfully. No convincing left inferior parathyroid gland was identified however palpation revealed a 1 cm mass just medial to carotid artery. This was excised as probable ectopic parathyroid gland. She was discharged two days later. Thirteen days postoperatively she attended Eye Casualty with a left-sided Horner's syndrome. A CT angio of aortic arch was normal. She was reviewed at ENT outpatients. Histopathology report of the expected ectopic parathyroid gland returned as benign ganglioneuroma, likely arising from her left sympathetic chain. Horner's syndrome is a common side effect from excision of ganglioneuromas, but an incredibly rare side effect from thyroid or parathyroid surgery.
Keywords: ear, nose and throat/otolaryngology; head and neck surgery; otolaryngology/ENT; thyroid disease.
© BMJ Publishing Group Limited 2020. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Katılmış H, Öztürkcan S, Adadan I, et al. . Cervical ganglioneuroma. Int J Pediatr Otorhinolaryngol Extra 2006;1:157–9. 10.1016/j.pedex.2006.04.006 - DOI
-
- Cavanaugh DA, Jawahar A, Harper J, et al. . Cervical ganglioneuroma in an adult man: case report and literature review of a rare occurrence. J La State Med Soc 2010;162:218–21. - PubMed
-
- Califano L, Zupi A, Mangone GM, et al. . Cervical ganglioneuroma: report of a case. Otolarynology Head Neck Surg 2001;124:115–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous