

Elevated circulating CD14++CD16+ intermediate monocytes are independently associated with extracardiac complications after cardiac surgery
- PMID: 31969629
- PMCID: PMC6976615
- DOI: 10.1038/s41598-020-57700-9
Elevated circulating CD14++CD16+ intermediate monocytes are independently associated with extracardiac complications after cardiac surgery
Abstract
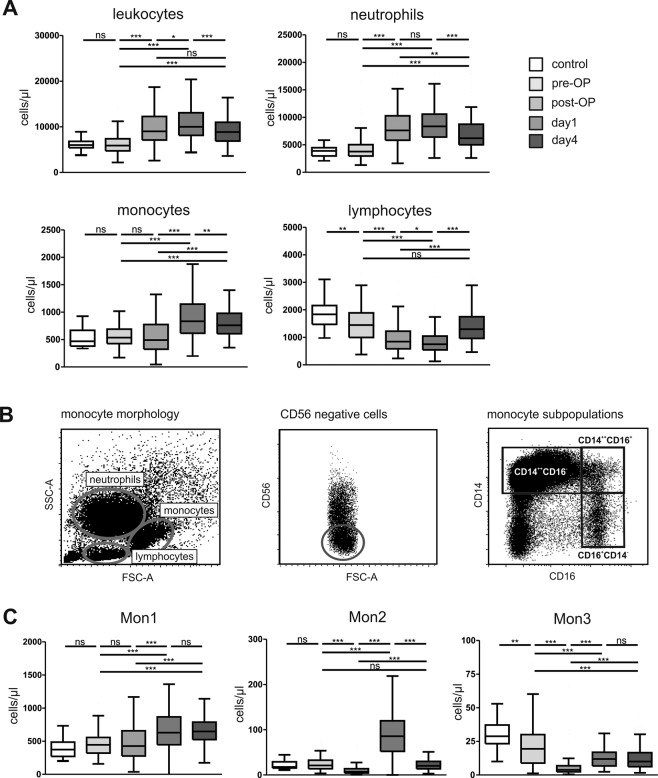
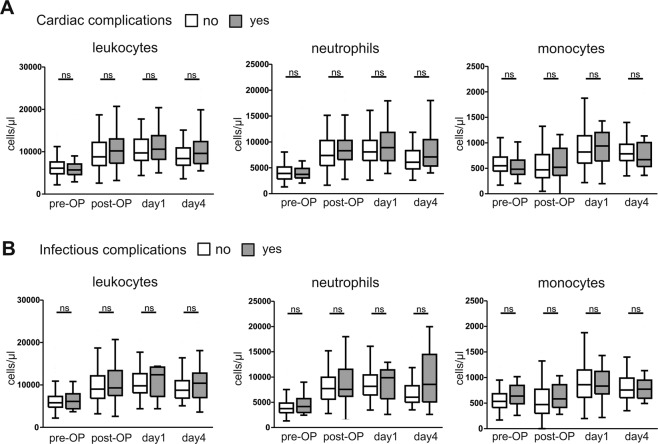
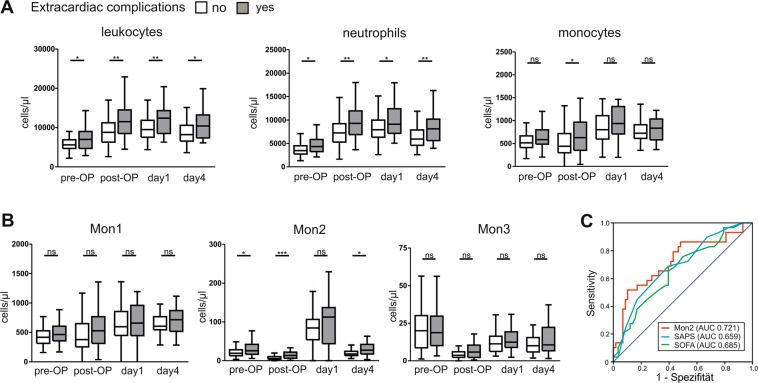
Elective cardiac surgery has low procedural complications. However, about 40% of patients develop extracardiac complications including delirium and acute kidney injury. We hypothesized that inflammatory processes and immune cell activation might be associated with these complications. We therefore prospectively included 104 patients undergoing cardiac surgery in our study. We assessed peripheral blood leukocyte populations by flow cytometry and circulating cytokines before operation, after surgery and at days one and four post-operatively. Patients undergoing cardiac surgery showed significantly elevated leukocytes and neutrophils after surgery. On the contrary, monocytes decreased after surgery and significantly increased at days 1 and 4, particularly classical (Mon1,CD14++CD16-) and intermediate (Mon2,CD14++CD16+) monocytes. While peripheral leukocyte subsets were unaltered in patients with infectious (n = 15) or cardiac complications (n = 31), post-operative leukocytes (p = 0.0016), neutrophils (p = 0.0061) and Mon2 (p = 0.0007) were clearly raised in patients developing extracardiac complications (n = 35). Using multiple logistic regression analyses, patient's age, ICU days, number of blood transfusions and elevated post-surgery Mon2 independently predicted extracardiac complications. Our findings demonstrate that elevated Mon2 after cardiac surgery are associated with an increased risk for extracardiac complications. These findings might improve the risk estimation after cardiac operations and the role of Mon2 for inflammation in cardiac surgery.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
