

Inflammation and fibrosis in chronic liver diseases including non-alcoholic fatty liver disease and hepatitis C
- PMID: 31969775
- PMCID: PMC6962431
- DOI: 10.3748/wjg.v26.i2.109
Inflammation and fibrosis in chronic liver diseases including non-alcoholic fatty liver disease and hepatitis C
Abstract
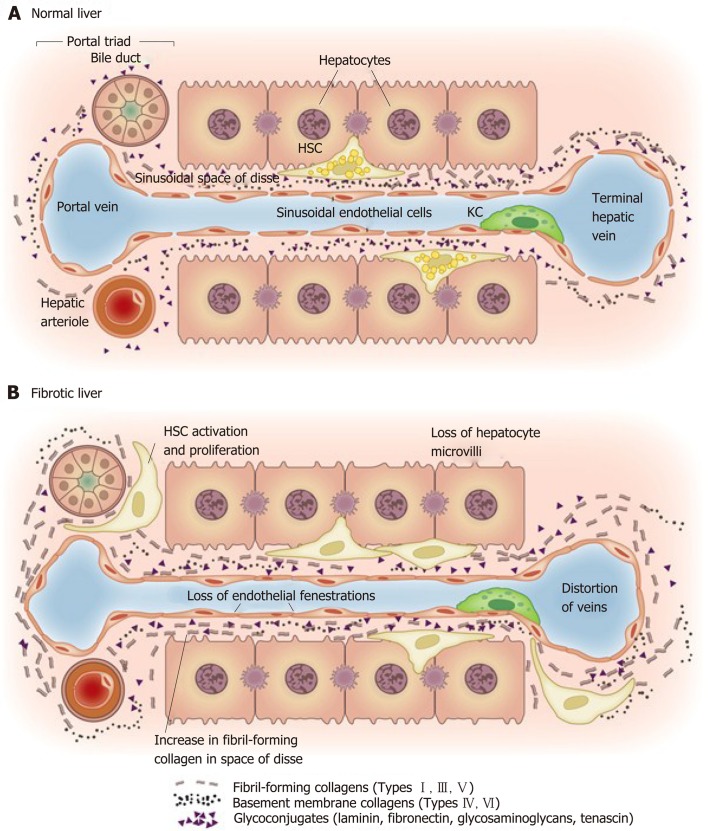
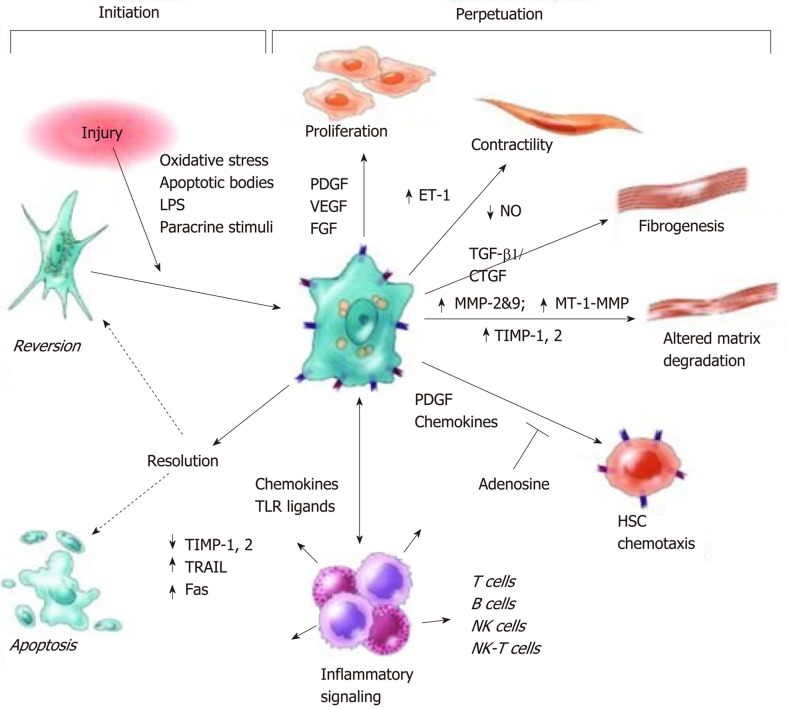
At present chronic liver disease (CLD), the third commonest cause of premature death in the United Kingdom is detected late, when interventions are ineffective, resulting in considerable morbidity and mortality. Injury to the liver, the largest solid organ in the body, leads to a cascade of inflammatory events. Chronic inflammation leads to the activation of hepatic stellate cells that undergo trans-differentiation to become myofibroblasts, the main extra-cellular matrix producing cells in the liver; over time increased extra-cellular matrix production results in the formation of liver fibrosis. Although fibrogenesis may be viewed as having evolved as a "wound healing" process that preserves tissue integrity, sustained chronic fibrosis can become pathogenic culminating in CLD, cirrhosis and its associated complications. As the reference standard for detecting liver fibrosis, liver biopsy, is invasive and has an associated morbidity, the diagnostic assessment of CLD by non-invasive testing is attractive. Accordingly, in this review the mechanisms by which liver inflammation and fibrosis develop in chronic liver diseases are explored to identify appropriate and meaningful diagnostic targets for clinical practice. Due to differing disease prevalence and treatment efficacy, disease specific diagnostic targets are required to optimally manage individual CLDs such as non-alcoholic fatty liver disease and chronic hepatitis C infection. To facilitate this, a review of the pathogenesis of both conditions is also conducted. Finally, the evidence for hepatic fibrosis regression and the mechanisms by which this occurs are discussed, including the current use of antifibrotic therapy.
Keywords: Anti-fibrotic; Biomarker; Chronic hepatitis C; Chronic liver disease; Cirrhosis; Fibrosis; Liver inflammation; Non-alcoholic fatty liver disease.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Figures
References
-
- Bacon BR, O'Grady JG. 2006. Comprehensive Clinical Hepatology. Elsevier.
-
- Rosenberg W, Baldrick T, Tanwar S. Missouri: Elsevier; 2019. Liver Disease. Tietz textbook of clinical chemistry and molecular diagnostics; pp. 699–722.
-
- Bedossa P, Paradis V. Liver extracellular matrix in health and disease. J Pathol. 2003;200:504–515. - PubMed
-
- Schuppan D. Structure of the extracellular matrix in normal and fibrotic liver: collagens and glycoproteins. Semin Liver Dis. 1990;10:1–10. - PubMed
-
- Protzer U, Maini MK, Knolle PA. Living in the liver: hepatic infections. Nat Rev Immunol. 2012;12:201–213. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
