

High precision radiotherapy including intensity-modulated radiation therapy and pulsed-dose-rate brachytherapy for cervical cancer: a retrospective monoinstitutional study
- PMID: 31969909
- PMCID: PMC6964350
- DOI: 10.5114/jcb.2019.90478
High precision radiotherapy including intensity-modulated radiation therapy and pulsed-dose-rate brachytherapy for cervical cancer: a retrospective monoinstitutional study
Abstract
Purpose: To analyse the survival outcomes and toxicity profile of patients treated with pulsed-dose-rate (PDR) brachytherapy (BT) after intensity-modulated radiation therapy (IMRT) for uterine cervical cancer in a single institution.
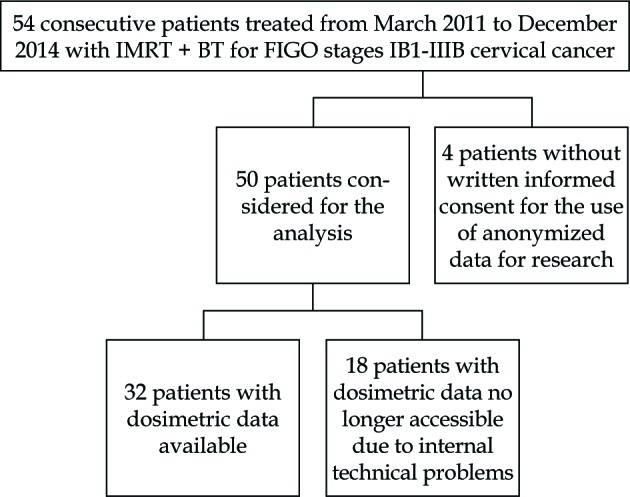
Material and methods: Between March 2011 and December 2014, 50 patients with histologically proven stages IB1-IVB cervical cancer were treated with IMRT followed by PDR-BT boost. Radiation treatment consisted of IMRT to pelvic with or without paraaortic lymph nodes to a total dose of 45-50.4 Gy. Weekly concomitant chemotherapy was administered to 45 patients. PDR-BT boost was delivered with a median dose of 30 Gy to the high-risk clinical target volume (HR-CTV) after a median time of 14 days since IMRT. Acute and late toxicity were evaluated by Radiation Therapy Oncology Group (RTOG) - European Organization for Research and Treatment of Cancer (EORTC) scoring criteria and Subjective Objective Management Analytic-Late Effects of Normal Tissues (SOMA-LENT) criteria.
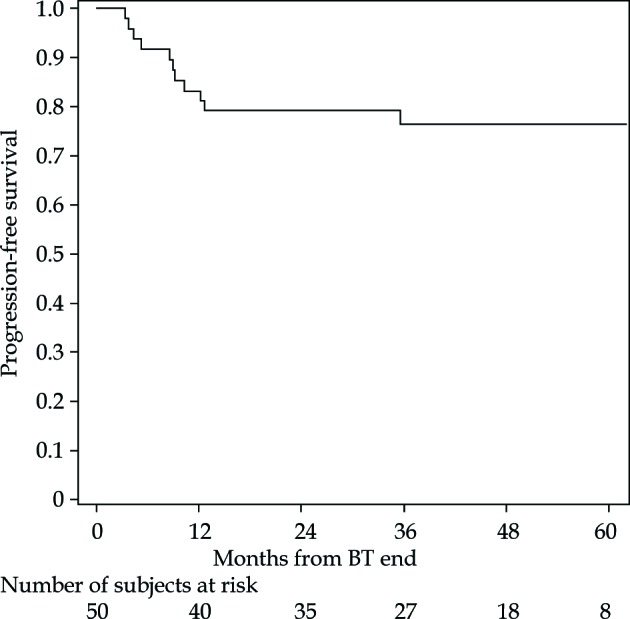
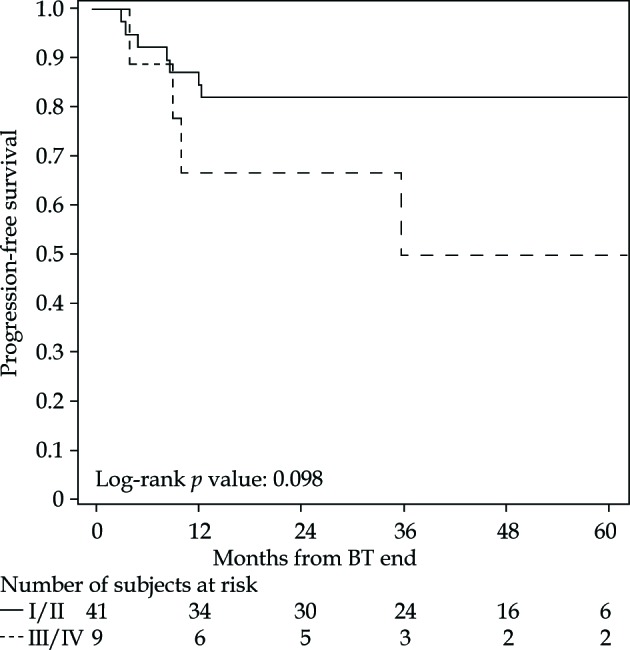
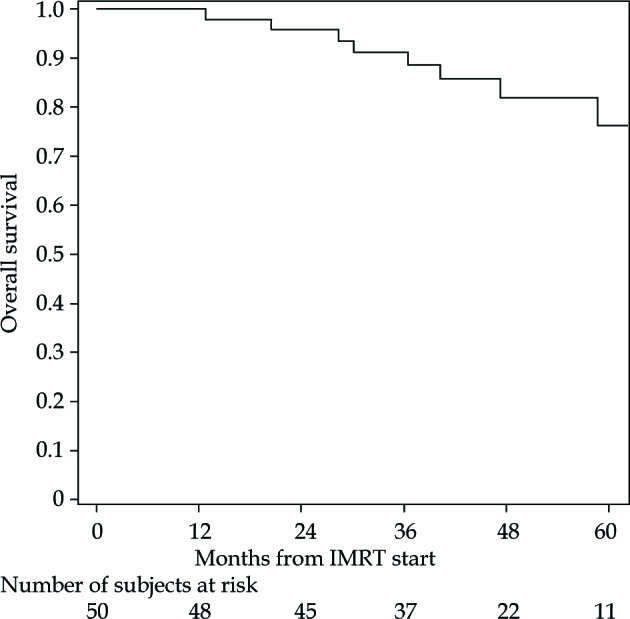
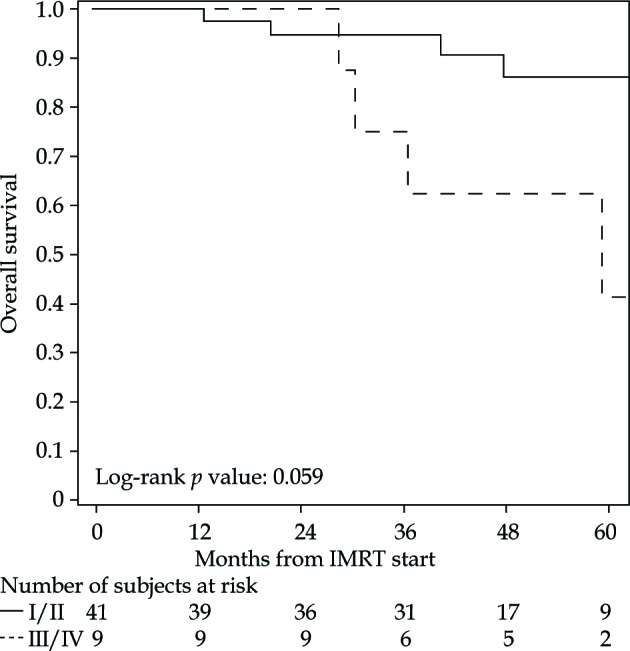
Results: Two patients had tumour persistence at 6 months after the end of BT. After a median follow-up of 33 months, 6 distant metastases with or without regional relapse were observed. The 1- and 5-year progression-free survival was 83% (95% CI: 69-91%) and 76% (95% CI: 61-86%), whereas the 3- and 5-year overall survival was 91% (95% CI: 78-97%) and 76% (95% CI: 56-88%), respectively. Urinary and rectal toxicity higher than grade 2 was observed in 6.3% and 17% of patients, respectively. Five patients (10.6%) had grade 4 gastrointestinal toxicity requiring colostomy.
Conclusions: Our study confirms that the combination of IMRT and PDR-BT can be considered an effective treatment for cervical cancer, ensuring high local control, despite the high percentage of locally advanced disease.
Keywords: IMRT; PDR; brachytherapy; cervical cancer.
Copyright © 2019 Termedia.
Figures
References
-
- Small W Jr, Bacon MA Bajaj A, et al. Cervical cancer: A global health crisis. Cancer 2017; 123: 2404-2412. - PubMed
-
- Tanderup K, Eifel PJ, Yashar CM et al. Curative radiation therapy for locally advanced cervical cancer: brachytherapy is not optional. Int J Radiat Oncol Biol Phys 2014; 88: 537-539. - PubMed
-
- Karlsson J, Dreifaldt AC, Mordhorst LB, Sorbe B. Differences in outcome for cervical cancer patients treated with or without brachytherapy. Brachytherapy 2017; 16: 133-140. - PubMed
-
- Holschneider CH, Petereit DG, Chu C et al. Brachytherapy: A critical component of primary radiation therapy for cervical cancer: From the Society of Gynecologic Oncology (SGO) and the American Brachytherapy Society (ABS). Brachytherapy 2019; 18: 123-132. - PubMed
-
- Naik A, Gurjar OP, Gupta KL et al. Comparison of dosimetric parameters and acute toxicity of intensity-modulated and three-dimensional radiotherapy in patients with cervix carcinoma: A randomized prospective study. Cancer Radiother 2016; 20: 370-376. - PubMed