

Reduced radiation-induced toxicity by using proton therapy for the treatment of oropharyngeal cancer
- PMID: 31971818
- PMCID: PMC7066974
- DOI: 10.1259/bjr.20190955
Reduced radiation-induced toxicity by using proton therapy for the treatment of oropharyngeal cancer
Abstract
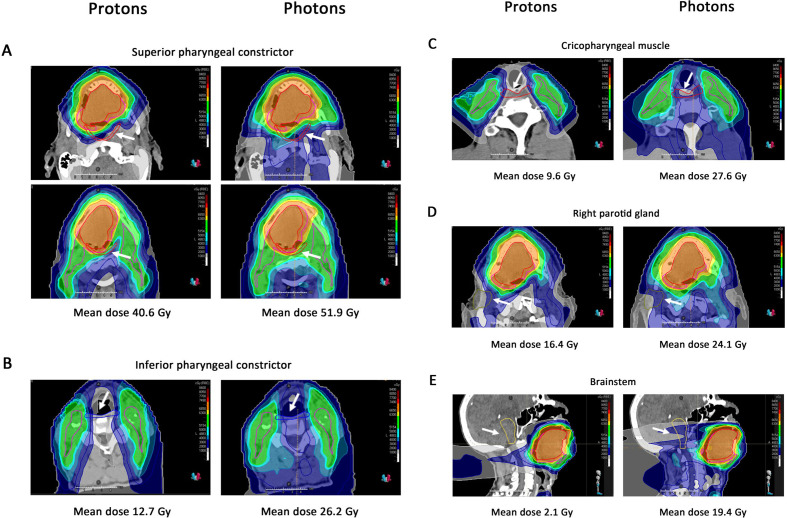
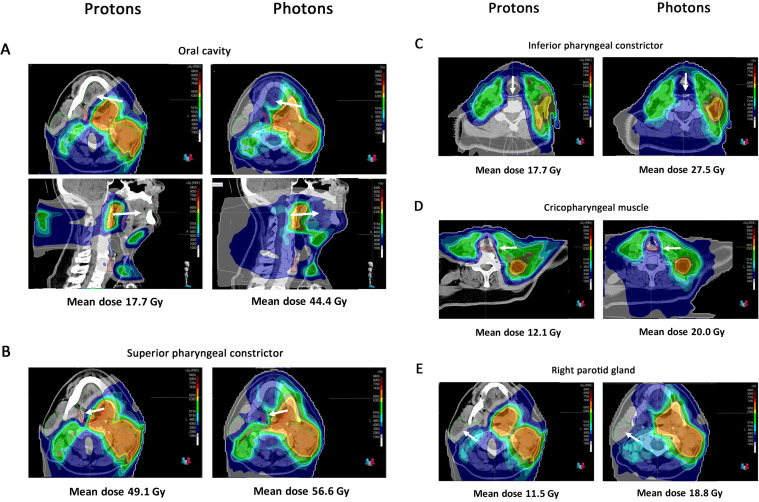
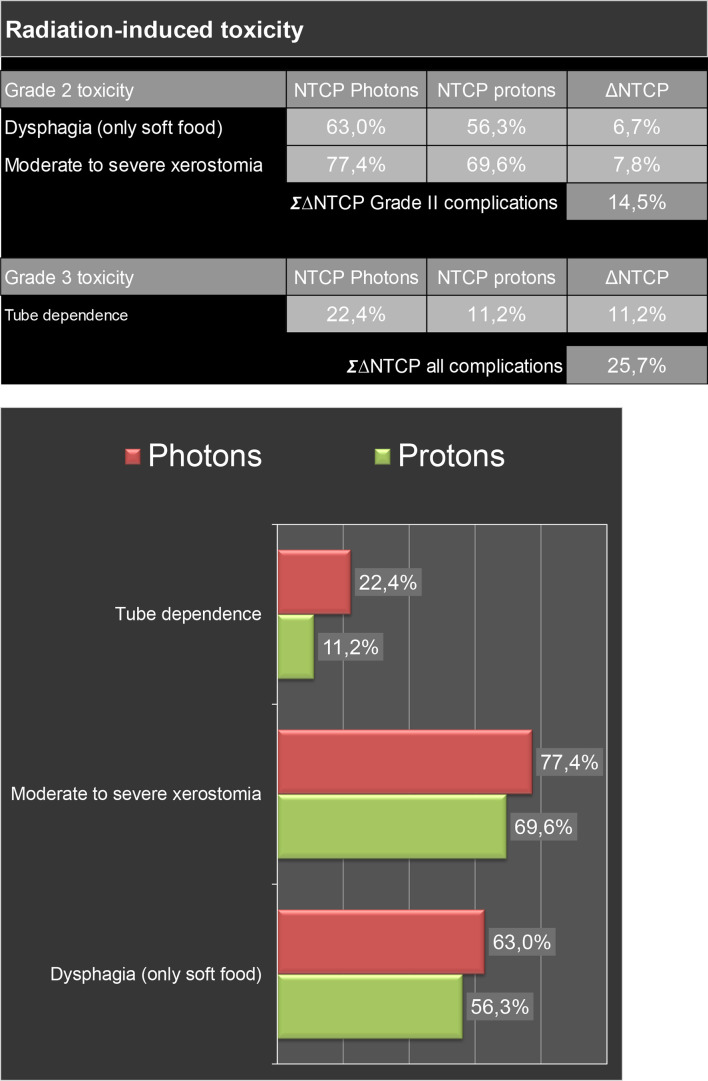
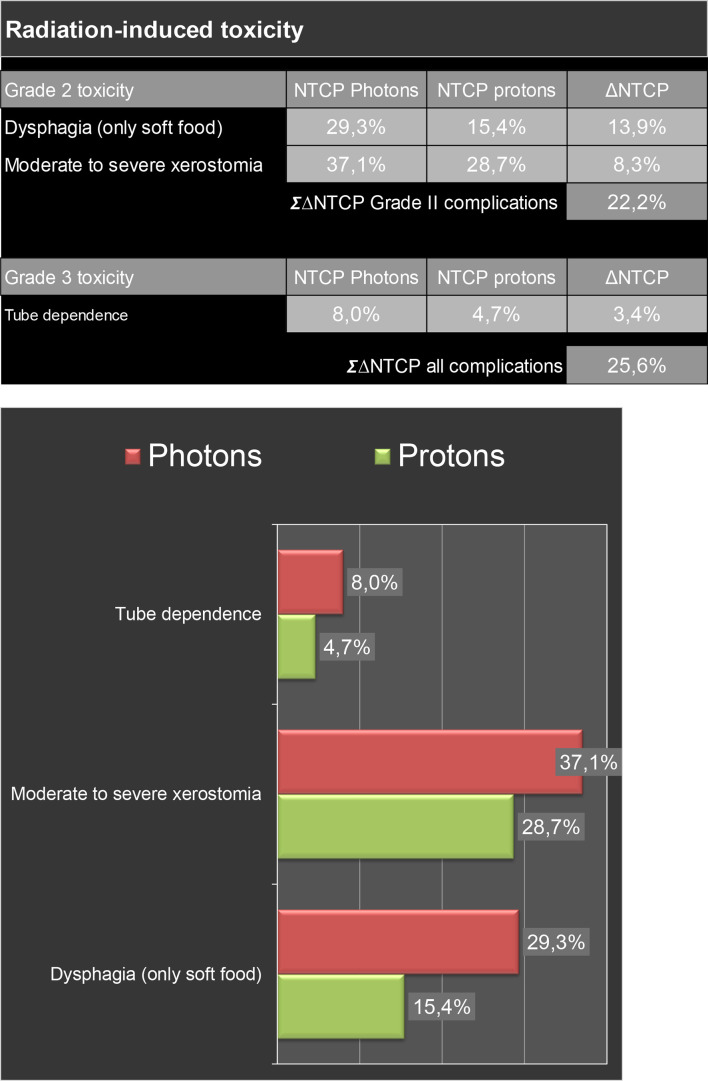
Patients with squamous cell carcinoma of the oropharynx are generally treated with (chemo) radiation. Patients with oropharyngeal cancer have better survival than patients with squamous cell carcinoma of other head and neck subsites, especially when related to human papillomavirus. However, radiotherapy results in a substantial percentage of survivors suffering from significant treatment-related side-effects. Late radiation-induced side-effects are mostly irreversible and may even be progressive, and particularly xerostomia and dysphagia affect health-related quality of life. As the risk of radiation-induced side-effects highly depends on dose to healthy normal tissues, prevention of radiation-induced xerostomia and dysphagia and subsequent improvement of health-relatedquality of life can be obtained by applying proton therapy, which offers the opportunity to reduce the dose to both the salivary glands and anatomic structures involved in swallowing.This review describes the results of the first cohort studies demonstrating that proton therapy results in lower dose levels in multiple organs at risk, which translates into reduced acute toxicity (i.e. up to 3 months after radiotherapy), while preserving tumour control. Next to reducing mucositis, tube feeding, xerostomia and distortion of the sense of taste, protons can improve general well-being by decreasing fatigue and nausea. Proton therapy results in decreased rates of tube feeding dependency and severe weight loss up to 1 year after radiotherapy, and may decrease the risk of radionecrosis of the mandible. Also, the model-based approach for selecting patients for proton therapy in the Netherlands is described in this review and future perspectives are discussed.
Figures
Similar articles
-
Using a reduced spot size for intensity-modulated proton therapy potentially improves salivary gland-sparing in oropharyngeal cancer.Int J Radiat Oncol Biol Phys. 2012 Feb 1;82(2):e313-9. doi: 10.1016/j.ijrobp.2011.05.005. Epub 2011 Jun 25. Int J Radiat Oncol Biol Phys. 2012. PMID: 21708427
-
Toxicities affecting quality of life after chemo-IMRT of oropharyngeal cancer: prospective study of patient-reported, observer-rated, and objective outcomes.Int J Radiat Oncol Biol Phys. 2013 Mar 15;85(4):935-40. doi: 10.1016/j.ijrobp.2012.08.030. Epub 2012 Oct 3. Int J Radiat Oncol Biol Phys. 2013. PMID: 23040224 Free PMC article.
-
Identification of Patient Benefit From Proton Therapy for Advanced Head and Neck Cancer Patients Based on Individual and Subgroup Normal Tissue Complication Probability Analysis.Int J Radiat Oncol Biol Phys. 2015 Aug 1;92(5):1165-1174. doi: 10.1016/j.ijrobp.2015.04.031. Epub 2015 Apr 23. Int J Radiat Oncol Biol Phys. 2015. PMID: 26194685
-
Correlation between plan quality improvements and reduced acute dysphagia and xerostomia in the definitive treatment of oropharyngeal squamous cell carcinoma.Head Neck. 2019 Apr;41(4):1096-1103. doi: 10.1002/hed.25594. Epub 2019 Jan 31. Head Neck. 2019. PMID: 30702180 Review.
-
[Proton therapy for head and neck squamous cell carcinomas: From physics to clinic].Cancer Radiother. 2019 Sep;23(5):439-448. doi: 10.1016/j.canrad.2019.05.015. Epub 2019 Jul 26. Cancer Radiother. 2019. PMID: 31358445 Review. French.
Cited by
-
Optimizing oropharyngeal cancer management by using proton beam therapy: trends of cost-effectiveness.BMC Cancer. 2021 Aug 21;21(1):944. doi: 10.1186/s12885-021-08638-2. BMC Cancer. 2021. PMID: 34419008 Free PMC article.
-
Immunomodulatory Effects of Radiotherapy.Int J Mol Sci. 2020 Oct 31;21(21):8151. doi: 10.3390/ijms21218151. Int J Mol Sci. 2020. PMID: 33142765 Free PMC article. Review.
-
Estimating the percentage of patients who might benefit from proton beam therapy instead of X-ray radiotherapy.Br J Radiol. 2022 May 1;95(1133):20211175. doi: 10.1259/bjr.20211175. Epub 2022 Mar 17. Br J Radiol. 2022. PMID: 35220723 Free PMC article.
-
The Role of Proton Therapy for Prostate Cancer in the Setting of Hip Prosthesis.Cancers (Basel). 2024 Jan 11;16(2):330. doi: 10.3390/cancers16020330. Cancers (Basel). 2024. PMID: 38254818 Free PMC article.
-
Proton therapy needs further technological development to fulfill the promise of becoming a superior treatment modality (compared to photon therapy).J Appl Clin Med Phys. 2021 Nov;22(11):4-11. doi: 10.1002/acm2.13450. Epub 2021 Nov 3. J Appl Clin Med Phys. 2021. PMID: 34730268 Free PMC article. No abstract available.
References
-
- Gupta T, Agarwal J, Jain S, Phurailatpam R, Kannan S, Ghosh-Laskar S, et al. . Three-Dimensional conformal radiotherapy (3D-CRT) versus intensity modulated radiation therapy (IMRT) in squamous cell carcinoma of the head and neck: a randomized controlled trial. Radiother Oncol 2012; 104: 343–8. doi: 10.1016/j.radonc.2012.07.001 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
