

Population-Based Surveillance for Birth Defects Potentially Related to Zika Virus Infection - 22 States and Territories, January 2016-June 2017
- PMID: 31971935
- PMCID: PMC7367037
- DOI: 10.15585/mmwr.mm6903a3
Population-Based Surveillance for Birth Defects Potentially Related to Zika Virus Infection - 22 States and Territories, January 2016-June 2017
Abstract
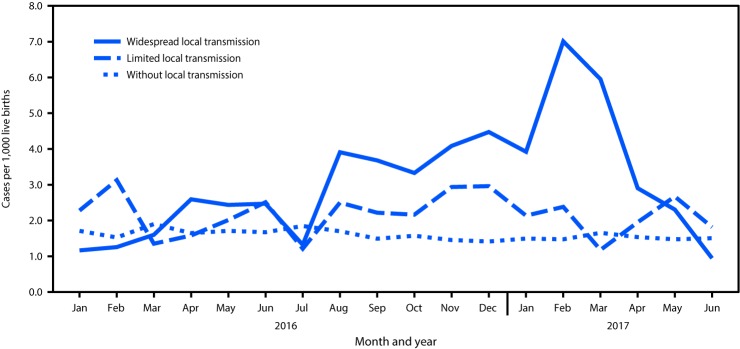
Zika virus infection during pregnancy can cause congenital brain and eye abnormalities and is associated with neurodevelopmental abnormalities (1-3). In areas of the United States that experienced local Zika virus transmission, the prevalence of birth defects potentially related to Zika virus infection during pregnancy increased in the second half of 2016 compared with the first half (4). To update the previous report, CDC analyzed population-based surveillance data from 22 states and territories to estimate the prevalence of birth defects potentially related to Zika virus infection, regardless of laboratory evidence of or exposure to Zika virus, among pregnancies completed during January 1, 2016-June 30, 2017. Jurisdictions were categorized as those 1) with widespread local transmission of Zika virus; 2) with limited local transmission of Zika virus; and 3) without local transmission of Zika virus. Among 2,004,630 live births, 3,359 infants and fetuses with birth defects potentially related to Zika virus infection during pregnancy were identified (1.7 per 1,000 live births, 95% confidence interval [CI] = 1.6-1.7). In areas with widespread local Zika virus transmission, the prevalence of birth defects potentially related to Zika virus infection during pregnancy was significantly higher during the quarters comprising July 2016-March 2017 (July-September 2016 = 3.0; October-December 2016 = 4.0; and January-March 2017 = 5.6 per 1,000 live births) compared with the reference period (January-March 2016) (1.3 per 1,000). These findings suggest a fourfold increase (prevalence ratio [PR] = 4.1, 95% CI = 2.1-8.4) in birth defects potentially related to Zika virus in widespread local transmission areas during January-March 2017 compared with that during January-March 2016, with the highest prevalence (7.0 per 1,000 live births) in February 2017. Population-based birth defects surveillance is critical for identifying infants and fetuses with birth defects potentially related to Zika virus regardless of whether Zika virus testing was conducted, especially given the high prevalence of asymptomatic disease. These data can be used to inform follow-up care and services as well as strengthen surveillance.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Rice ME, Galang RR, Roth NM, et al. Vital signs: Zika-associated birth defects and neurodevelopmental abnormalities possibly associated with congenital Zika virus infection—U.S. territories and freely associated states, 2018. MMWR Morb Mortal Wkly Rep 2018;67:858–67. 10.15585/mmwr.mm6731e1 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
