

The clinical benefit of instituting a prospective clinical community-acquired respiratory virus surveillance program in allogeneic hematopoietic stem cell transplantation
- PMID: 31972212
- PMCID: PMC7112613
- DOI: 10.1016/j.jinf.2019.12.022
The clinical benefit of instituting a prospective clinical community-acquired respiratory virus surveillance program in allogeneic hematopoietic stem cell transplantation
Abstract
Background: There is a lack of studies comparing clinical outcomes among retrospective versus prospective cohorts of allogeneic stem cell transplant (allo-HCT) recipients with community acquired respiratory virus (CARV) infections.
Methods: We compare outcomes in two consecutive cohorts of allo-HCT recipients with CARV infections. The retrospective cohort included 63 allo-HCT recipients with 108 CARV infections from January 2013 to April 2016 who were screened and managed following standard clinical practice based on influenza and respiratory syncytial virus rapid antigen detection methods. The prospective cohort was comprised of 144 consecutive recipients with 297 CARV episodes included in a prospective interventional clinical surveillance program (ProClinCarvSur-P) based on syndromic multiplex PCR as first-line test from May 2016 to December 2018 at a single transplant center.
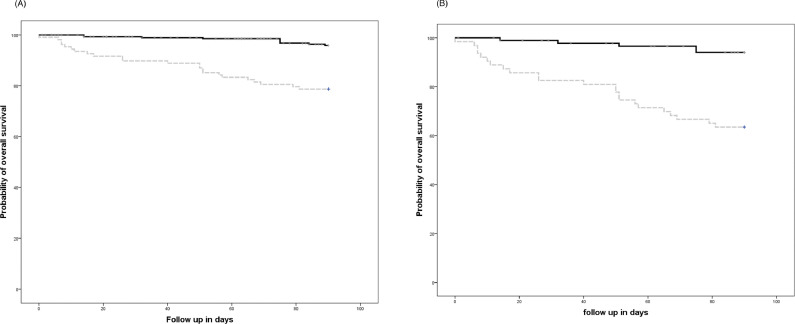
Results: CARV infections in the retrospective cohort showed more severe clinical features at the time of diagnosis compared to the prospective cohort (fever 83% vs. 57%, hospital admission 69% vs. 28% and lower respiratory tract 58% vs. 31%, respectively, p ≤ 0.002 for all comparisons). Antiviral therapy was more commonly prescribed in the prospective cohort (69 vs. 43 treated CARV episodes), particularly at the upper respiratory tract disease stage (34 vs. 12 treated CARV episodes). Three-month all-cause mortality was significantly higher in the retrospective cohort (n = 23, 37% vs. n = 10, 7%, p < 0.0001). Multivariate logistic regression analysis showed that recipients included in ProClinCarvSur-P had lower mortality rate [odds ratio 0.31, 95% confidence interval 0.12-0.7, p = 0.01].
Conclusion: This study report on outcome differences when reporting retrospective vs. prospective CARV infections after allo-HCT. Recipients included in a ProClinCarvSur-P had lower mortality.
Keywords: Allogeneic hematopoietic stem cell transplantation; Community-acquired respiratory virus; Immunodeficiency score index; Influenza; Parainfluenza virus; Prospective respiratory virus surveillance program; Respiratory syncytial virus; Respiratory virus infection.
Copyright © 2020. Published by Elsevier Ltd.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
The effect of timing on community acquired respiratory virus infection mortality during the first year after allogeneic hematopoietic stem cell transplantation: a prospective epidemiological survey.Bone Marrow Transplant. 2020 Feb;55(2):431-440. doi: 10.1038/s41409-019-0698-7. Epub 2019 Sep 24. Bone Marrow Transplant. 2020. PMID: 31551521 Free PMC article.
-
Incidence, risk factors, and outcome of pulmonary invasive fungal disease after respiratory virus infection in allogeneic hematopoietic stem cell transplantation recipients.Transpl Infect Dis. 2019 Oct;21(5):e13158. doi: 10.1111/tid.13158. Epub 2019 Sep 3. Transpl Infect Dis. 2019. PMID: 31402532 Free PMC article.
-
Community-Acquired Respiratory Virus Infections: A Threat to Long-Term survivors after Allogeneic Stem Cell Transplant?Clin Infect Dis. 2024 Dec 5:ciae602. doi: 10.1093/cid/ciae602. Online ahead of print. Clin Infect Dis. 2024. PMID: 39657017
-
Respiratory virus infections after allogeneic stem cell transplantation: Current understanding, knowledge gaps, and recent advances.Transpl Infect Dis. 2023 Nov;25 Suppl 1:e14117. doi: 10.1111/tid.14117. Epub 2023 Aug 16. Transpl Infect Dis. 2023. PMID: 37585370 Review.
-
Correlation of initial upper respiratory tract viral burden with progression to lower tract disease in adult allogeneic hematopoietic cell transplant recipients.J Clin Virol. 2022 Jun;150-151:105152. doi: 10.1016/j.jcv.2022.105152. Epub 2022 Apr 4. J Clin Virol. 2022. PMID: 35447514 Free PMC article. Review.
Cited by
-
Identification of 1,2,3-triazole-phthalimide derivatives as potential drugs against COVID-19: a virtual screening, docking and molecular dynamic study.J Biomol Struct Dyn. 2022 Aug;40(12):5462-5480. doi: 10.1080/07391102.2020.1871073. Epub 2021 Jan 18. J Biomol Struct Dyn. 2022. PMID: 33459182 Free PMC article.
-
Incidence and impact of community respiratory viral infections in post-transplant cyclophosphamide-based graft-versus-host disease prophylaxis and haploidentical stem cell transplantation.Br J Haematol. 2021 Jul;194(1):145-157. doi: 10.1111/bjh.17563. Epub 2021 Jun 14. Br J Haematol. 2021. PMID: 34124796 Free PMC article.
-
The pulmonary metatranscriptome prior to pediatric HCT identifies post-HCT lung injury.Blood. 2021 Mar 25;137(12):1679-1689. doi: 10.1182/blood.2020009246. Blood. 2021. PMID: 33512420 Free PMC article.
References
-
- US Centers for Disease Control and Prevention. 2018. Flu activity & surveillance. https://www.cdc.gov/flu/weekly/fluactivitysurv.htm.
-
- Red nacional de vigilancia epidemiológica. Instituto de salud Carlos III. Boletín Epidemiológico Semanal eISSN: 2173-9277. https://revistas.isciii.es
-
- European Centre for Disease Prevention and Control/WHO Regional Office for Europe. Flu News Europe, Joint ECDC–WHO. https://flunewseurope.org.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
