

Differences in Aortopathy in Patients with a Bicuspid Aortic Valve with or without Aortic Coarctation
- PMID: 31972995
- PMCID: PMC7073528
- DOI: 10.3390/jcm9020290
Differences in Aortopathy in Patients with a Bicuspid Aortic Valve with or without Aortic Coarctation
Abstract
Objective: The combination of aortic coarctation (CoA) and bicuspid aortic valve (BAV) is assumed to be associated with a higher risk of ascending aortic dilatation and type A dissection, and current European Society of Cardiology (ESC) guidelines advise therefore to operate at a lower threshold in the presence of CoA. The aim of our study is to evaluate whether the coexistence of CoA in BAV patients is indeed associated with a higher risk of ascending aortic events (AAE).
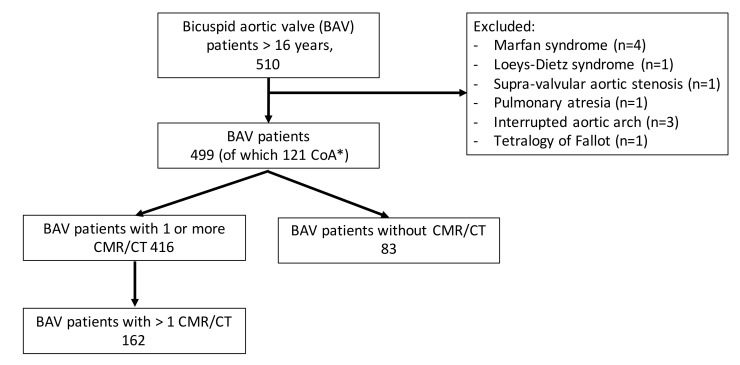
Methods: In a retrospective study, all adult BAV patients visiting the outpatient clinic of our tertiary care center between February 2003 and February 2019 were included. The primary end point was an ascending aortic event (AAE) defined as ascending aortic dissection/rupture or preventive surgery. The secondary end points were aortic dilatation and aortic growth.
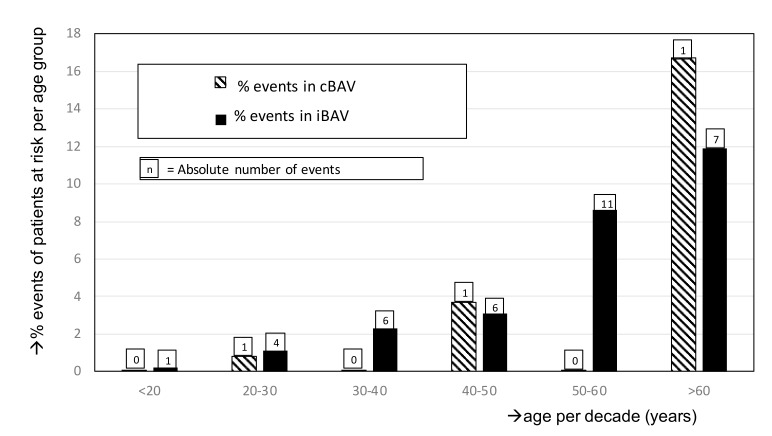
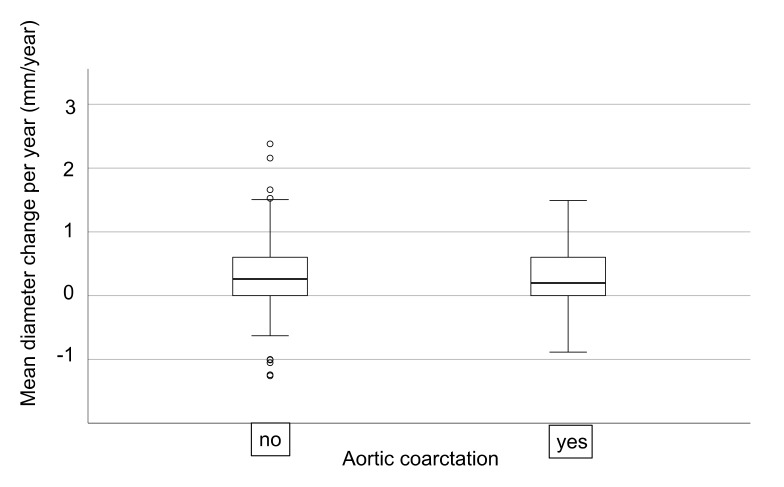
Results: In total, 499 BAV patients (43.7% female, age 40.3 ± 15.7 years) were included, of which 121 (24%) had a history of CoA (cBAV). An aortic event occurred in 38 (7.6%) patients at a mean age of 49.0 ± 13.6 years. In the isolated BAV group (iBAV), significantly more AAE occurred, but this was mainly driven by aortic valve dysfunction as indication for aortic surgery. There was no significant difference in the occurrence of dissection or severely dilated ascending aorta (>50mm) between the iBAV and cBAV patients (p = 0.56). The aortic diameter was significantly smaller in the cBAV group (30.3 ± 6.9 mm versus 35.7 ± 7.6 mm; p < 0.001). The median aortic diameter increase was 0.23 (interquartile range (IQR): 0.0-0.67) mm/year and was not significantly different between both groups (p = 0.74).
Conclusion: Coexistence of CoA in BAV patients was not associated with a higher risk of aortic dissection, preventive aortic surgery, aortic dilatation, or more rapid aorta growth. This study suggests that CoA is not a risk factor in BAV patients, and the advice to operate at lower diameter should be reevaluated.
Keywords: Bicuspid aortic valve; aortic coarctation; aortic dilation; aortic dissection; cardiac magnetic resonance imaging; congenital heart disease.
Conflict of interest statement
The authors declare no conflict of interest
Figures
References
-
- Oliver J.M., Alonso-Gonzalez R., Gonzalez A.E., Gallego P., Sánchez-Recalde A., Cuesta E., Aroca A., López-Sendon J.L. Risk of Aortic Root or Ascending Aorta Complications in Patients With Bicuspid Aortic Valve With and Without Coarctation of the Aorta. Am. J. Cardiol. 2009;104:1001–1006. doi: 10.1016/j.amjcard.2009.05.045. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
