

Estimating Myocardial Infarction Size With a Simple Electrocardiographic Marker Score
- PMID: 31973600
- PMCID: PMC7033860
- DOI: 10.1161/JAHA.119.014205
Estimating Myocardial Infarction Size With a Simple Electrocardiographic Marker Score
Abstract
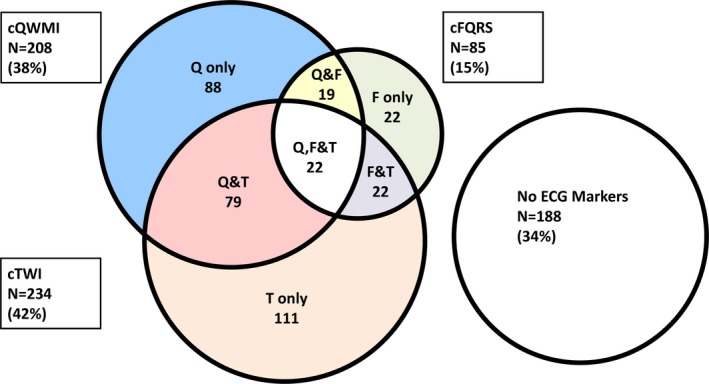
Background Myocardial infarction (MI) size is a key predictor of prognosis in post-MI patients. Cardiovascular magnetic resonance (CMR) is the gold standard test for MI quantification, but the ECG is less expensive and more widely available. We sought to quantify the relationship between ECG markers and cardiovascular magnetic resonance infarct size. Methods and Results Patients with prior MI enrolled in the DETERMINE (Defibrillators to Reduce Risk by Magnetic Resonance Imaging Evaluation) and PRE-DETERMINE Trial and Registry were included. ECG leads were analyzed for markers of MI: Q waves, fragmented QRS, and T wave inversion. DETERMINE Score=number of leads with [Q waves×2]+[fragmented QRS]+[T wave inversion]. Left ventricular ejection fraction (LVEF) and infarct size as a percentage of left ventricular mass (MI%) were quantified by cardiovascular magnetic resonance. The Modified Selvester Score estimates MI size from 37 ECG criteria. In 551 patients (aged 62.1±10.9 years, 79% men, and LVEF=40.3±11.0%), MI% increased as the number of ECG markers increased (P<0.001). By univariable linear regression, the DETERMINE Score (range 0-26) estimated MI% (R2=0.18, P<0.001) with an accuracy approaching that of LVEF (R2=0.22, P<0.001) and higher than the Modified Selvester Score (R2=0.09, P<0.001). By multivariable linear regression, addition of the DETERMINE Score improved estimation of MI% over LVEF alone (P<0.001) and over Modified Selvester Score alone (P<0.001). Conclusions In patients with prior MI, a simple ECG score estimates infarct size and improves infarct size estimation over LVEF alone. Because infarct size is a powerful prognostic indicator, the DETERMINE Score holds promise as a simple and inexpensive risk assessment tool.
Keywords: electrocardiography; magnetic resonance imaging; myocardial infarction; prognosis; sudden death.
Figures




References
-
- El Aidi H, Adams A, Moons KG, Den Ruijter HM, Mali WP, Doevendans PA, Nagel E, Schalla S, Bots ML, Leiner T. Cardiac magnetic resonance imaging findings and the risk of cardiovascular events in patients with recent myocardial infarction or suspected or known coronary artery disease: a systematic review of prognostic studies. J Am Coll Cardiol. 2014;63:1031–1045. - PubMed
-
- Lee DC, Goldberger JJ. CMR for sudden cardiac death risk stratification: are we there yet? JACC Cardiovasc Imaging. 2013;6:345–348. - PubMed
-
- Schelbert EB, Cao JJ, Sigurdsson S, Aspelund T, Kellman P, Aletras AH, Dyke CK, Thorgeirsson G, Eiriksdottir G, Launer LJ, Gudnason V, Harris TB, Arai AE. Prevalence and prognosis of unrecognized myocardial infarction determined by cardiac magnetic resonance in older adults. JAMA. 2012;308:890–896. - PMC - PubMed
-
- Wu E, Ortiz JT, Tejedor P, Lee DC, Bucciarelli‐Ducci C, Kansal P, Carr JC, Holly TA, Lloyd‐Jones D, Klocke FJ, Bonow RO. Infarct size by contrast enhanced cardiac magnetic resonance is a stronger predictor of outcomes than left ventricular ejection fraction or end‐systolic volume index: prospective cohort study. Heart. 2008;94:730–736. - PubMed
-
- Das MK, Khan B, Jacob S, Kumar A, Mahenthiran J. Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation. 2006;113:2495–2501. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
