

Health comorbidities and cognitive abilities across the lifespan in Down syndrome
- PMID: 31973697
- PMCID: PMC6979347
- DOI: 10.1186/s11689-019-9306-9
Health comorbidities and cognitive abilities across the lifespan in Down syndrome
Abstract
Background: Down syndrome (DS) is associated with variable intellectual disability and multiple health and psychiatric comorbidities. The impact of such comorbidities on cognitive outcomes is unknown. We aimed to describe patterns of physical health and psychiatric comorbidity prevalence, and receptive language ability, in DS across the lifespan, and determine relationships with cognitive outcomes.
Methods: Detailed medical histories were collected and cognitive abilities measured using standardised tests for 602 individuals with DS from England and Wales (age range 3 months to 73 years). Differences in prevalence rates between age groups and between males and females were determined using chi-squared or Fisher's exact tests. In adults, rates for psychiatric comorbidities were compared to expected population rates using standardised morbidity ratios (SMRs). Adapted ANCOVA functions were constructed to explore age and sex associations with receptive language ability across the lifespan, and regression analyses were performed to determine whether the presence of health comorbidities or physical phenotypes predicted cognitive abilities.
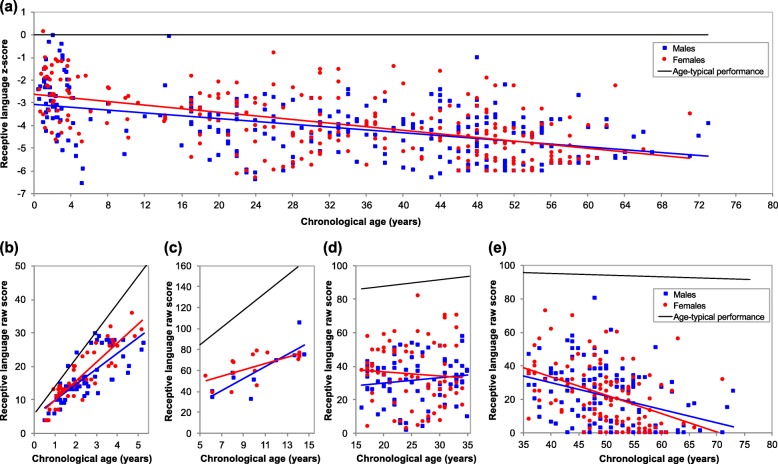
Results: Multiple comorbidities showed prevalence differences across the lifespan, though there were few sex differences. In adults, SMRs were increased in males and decreased in females with DS for schizophrenia, bipolar disorder, and anxiety. Further, SMRs were increased in both males and females with DS for dementia, autism, ADHD, and depression, with differences more pronounced in females for dementia and autism, and in males for depression. Across the lifespan, receptive language abilities increasingly deviated from age-typical levels, and males scored poorer than females. Only autism and epilepsy were associated with poorer cognitive ability in those aged 16-35 years, with no relationships for physical health comorbidities, including congenital heart defects.
Conclusions: Our results indicate the prevalence of multiple comorbidities varies across the lifespan in DS, and in adults, rates for psychiatric comorbidities show different patterns for males and females relative to expected population rates. Further, most health comorbidities are not associated with poorer cognitive outcomes in DS, apart from autism and epilepsy. It is essential for clinicians to consider such differences to provide appropriate care and treatment for those with DS and to provide prognostic information relating to cognitive outcomes in those with comorbidities.
Keywords: Cognitive outcomes; Down syndrome; Health comorbidities; Intellectual disability; Psychiatric comorbidities; Receptive language ability.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
