

Systematic assessment of fluid responsiveness during early septic shock resuscitation: secondary analysis of the ANDROMEDA-SHOCK trial
- PMID: 31973735
- PMCID: PMC6979284
- DOI: 10.1186/s13054-020-2732-y
Systematic assessment of fluid responsiveness during early septic shock resuscitation: secondary analysis of the ANDROMEDA-SHOCK trial
Abstract
Background: Fluid boluses are administered to septic shock patients with the purpose of increasing cardiac output as a means to restore tissue perfusion. Unfortunately, fluid therapy has a narrow therapeutic index, and therefore, several approaches to increase safety have been proposed. Fluid responsiveness (FR) assessment might predict which patients will effectively increase cardiac output after a fluid bolus (FR+), thus preventing potentially harmful fluid administration in non-fluid responsive (FR-) patients. However, there are scarce data on the impact of assessing FR on major outcomes. The recent ANDROMEDA-SHOCK trial included systematic per-protocol assessment of FR. We performed a post hoc analysis of the study dataset with the aim of exploring the relationship between FR status at baseline, attainment of specific targets, and clinically relevant outcomes.
Methods: ANDROMEDA-SHOCK compared the effect of peripheral perfusion- vs. lactate-targeted resuscitation on 28-day mortality. FR was assessed before each fluid bolus and periodically thereafter. FR+ and FR- subgroups, independent of the original randomization, were compared for fluid administration, achievement of resuscitation targets, vasoactive agents use, and major outcomes such as organ dysfunction and support, length of stay, and 28-day mortality.
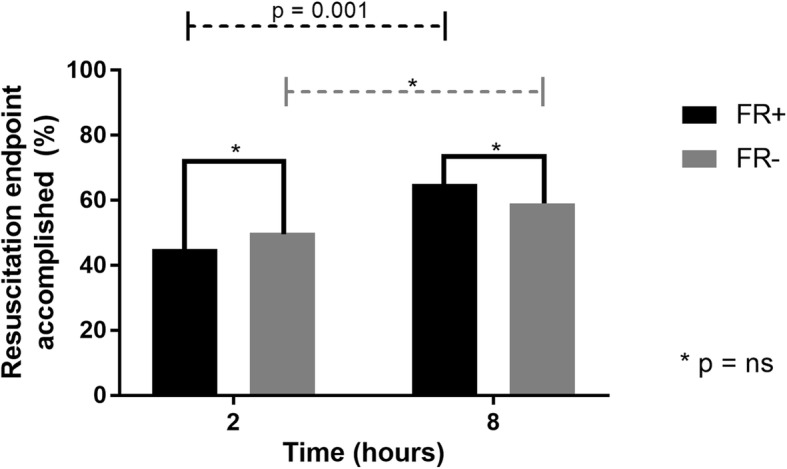
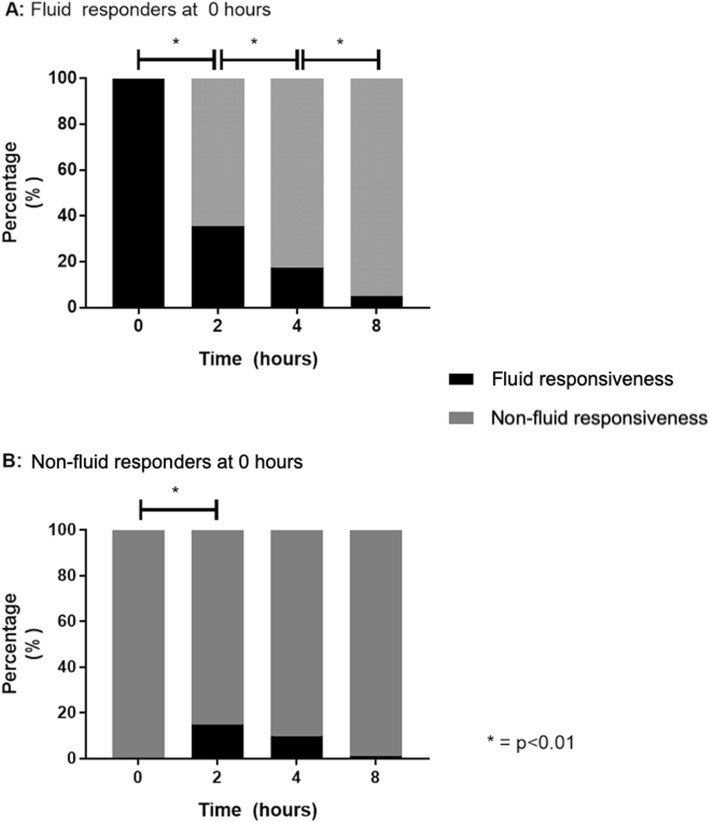
Results: FR could be determined in 348 patients at baseline. Two hundred and forty-two patients (70%) were categorized as fluid responders. Both groups achieved comparable successful resuscitation targets, although non-fluid responders received less resuscitation fluids (0 [0-500] vs. 1500 [1000-2500] mL; p 0.0001), exhibited less positive fluid balances, but received more vasopressor testing. No difference in clinically relevant outcomes between FR+ and FR- patients was found, including 24-h SOFA score (9 [5-12] vs. 8 [5-11], p = 0.4), need for MV (78% vs. 72%, p = 0.16), need for RRT (18% vs. 21%, p = 0.7), ICU-LOS (6 [3-11] vs. 6 [3-16] days, p = 0.2), and 28-day mortality (40% vs. 36%, p = 0.5). Only thirteen patients remained fluid responsive along the intervention period.
Conclusions: Systematic assessment allowed determination of fluid responsiveness status in more than 80% of patients with early septic shock. Fluid boluses could be stopped in non-fluid responsive patients without any negative impact on clinical relevant outcomes. Our results suggest that fluid resuscitation might be safely guided by FR assessment in septic shock patients.
Trial registration: ClinicalTrials.gov identifier, NCT03078712. Registered retrospectively on March 13, 2017.
Keywords: Early resuscitation; Fluid overload; Fluid responsiveness; Septic shock.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of a Resuscitation Strategy Targeting Peripheral Perfusion Status vs Serum Lactate Levels on 28-Day Mortality Among Patients With Septic Shock: The ANDROMEDA-SHOCK Randomized Clinical Trial.JAMA. 2019 Feb 19;321(7):654-664. doi: 10.1001/jama.2019.0071. JAMA. 2019. PMID: 30772908 Free PMC article. Clinical Trial.
-
Early goal-directed therapy using a physiological holistic view: the ANDROMEDA-SHOCK-a randomized controlled trial.Ann Intensive Care. 2018 Apr 23;8(1):52. doi: 10.1186/s13613-018-0398-2. Ann Intensive Care. 2018. PMID: 29687277 Free PMC article.
-
Effects of a Resuscitation Strategy Targeting Peripheral Perfusion Status versus Serum Lactate Levels among Patients with Septic Shock. A Bayesian Reanalysis of the ANDROMEDA-SHOCK Trial.Am J Respir Crit Care Med. 2020 Feb 15;201(4):423-429. doi: 10.1164/rccm.201905-0968OC. Am J Respir Crit Care Med. 2020. PMID: 31574228
-
Is There an Optimum Duration of Fluid Bolus in Pediatric Septic Shock? A Critical Appraisal of "Fluid Bolus Over 15-20 Versus 5-10 Minutes Each in the First Hour of Resuscitation in Children With Septic Shock: A Randomized Controlled Trial" by Sankar et al (Pediatr Crit Care Med 2017; 18:e435-e445).Pediatr Crit Care Med. 2018 Apr;19(4):369-371. doi: 10.1097/PCC.0000000000001459. Pediatr Crit Care Med. 2018. PMID: 29369077 Review.
-
The initial resuscitation of septic shock.J Crit Care. 2020 Jun;57:108-117. doi: 10.1016/j.jcrc.2020.02.004. Epub 2020 Feb 11. J Crit Care. 2020. PMID: 32135409 Review.
Cited by
-
Recent trends in septic shock management: a narrative review of current evidence and recommendations.Ann Med Surg (Lond). 2024 May 15;86(8):4532-4540. doi: 10.1097/MS9.0000000000002048. eCollection 2024 Aug. Ann Med Surg (Lond). 2024. PMID: 39118750 Free PMC article. Review.
-
Assessing fluid responsiveness with ultrasound in the neonatal intensive care setting: the mini-fluid challenge.Eur J Pediatr. 2024 Apr;183(4):1947-1951. doi: 10.1007/s00431-024-05425-6. Epub 2024 Jan 26. Eur J Pediatr. 2024. PMID: 38276998 Free PMC article.
-
The time cost of physiologically ineffective intravenous fluids in the emergency department: an observational pilot study employing wearable Doppler ultrasound.J Intensive Care. 2023 Feb 15;11(1):7. doi: 10.1186/s40560-023-00655-6. J Intensive Care. 2023. PMID: 36793079 Free PMC article.
-
Characteristics of resuscitation, and association between use of dynamic tests of fluid responsiveness and outcomes in septic patients: results of a multicenter prospective cohort study in Argentina.Ann Intensive Care. 2020 Apr 15;10(1):40. doi: 10.1186/s13613-020-00659-7. Ann Intensive Care. 2020. PMID: 32297028 Free PMC article.
-
A proof of concept for microcirculation monitoring using machine learning based hyperspectral imaging in critically ill patients: a monocentric observational study.Crit Care. 2024 Jul 10;28(1):230. doi: 10.1186/s13054-024-05023-w. Crit Care. 2024. PMID: 38987802 Free PMC article.
References
-
- Malbrain MLNG, Van Regenmortel N, Saugel B, De Tavernier B, Van Gaal PJ, Joannes-Boyau O, et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D’s and the four phases of fluid therapy. Ann Intensive Care. 2018;8:66. doi: 10.1186/s13613-018-0402-x. - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
