

Dosimetry after peptide receptor radionuclide therapy: impact of reduced number of post-treatment studies on absorbed dose calculation and on patient management
- PMID: 31975156
- PMCID: PMC6977807
- DOI: 10.1186/s40658-020-0273-8
Dosimetry after peptide receptor radionuclide therapy: impact of reduced number of post-treatment studies on absorbed dose calculation and on patient management
Abstract
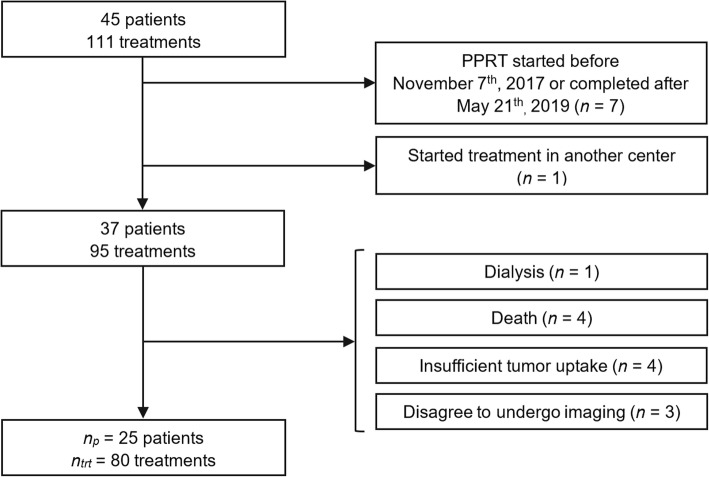
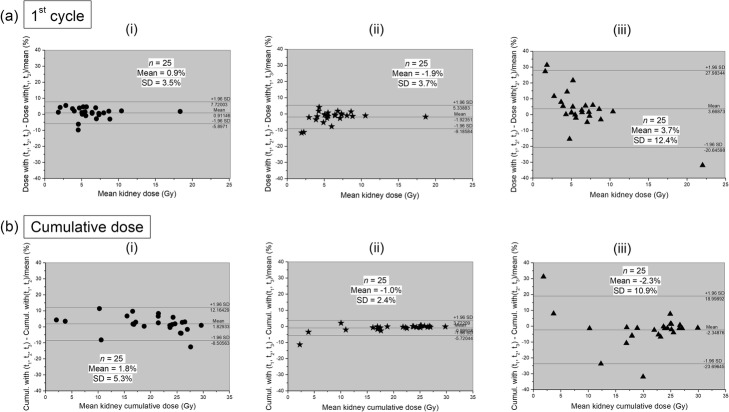
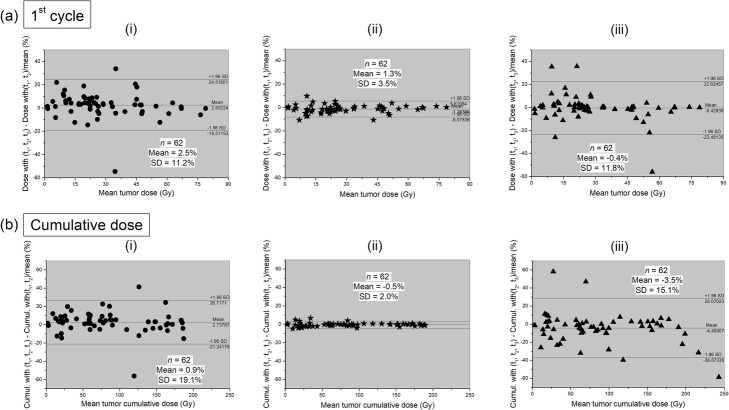
Background: After each cycle of [177Lu]-DOTA-TATE peptide receptor radionuclide therapy (PRRT) dosimetry is performed to enable precise calculation of the radiation-absorbed dose to tumors and normal organs. Absorbed doses are routinely calculated from three quantitative single-photon emission computed tomography (SPECT) studies corrected by computed tomography (CT) acquired at t1 = 24 h, t2 = 96 h, and t3 = 168 h after the first cycle of treatment. After following cycles, a single SPECT/CT study is performed. The aim of the present study is to assess the feasibility of a "two time point" quantitative SPECT/CT protocol after the first PRRT cycle and its impact on patient management. Quantitative SPECT/CT data of 25 consecutive patients with metastatic neuroendocrine tumors after PRRT were retrospectively analyzed. Radiation-absorbed doses calculated using the standard protocol with three SPECT/CT studies acquired at (t1, t2, t3) were compared to those obtained from three different "two time point" protocols with SPECT/CT studies performed at (t1, t2), (t1, t3), or (t2, t3).
Results: The best agreement for the cumulative doses absorbed by the kidneys, bone marrow, liver, spleen, and tumors with the conventional protocol was obtained with the (t1, t3) protocol with mean relative differences of - 1.0% ± 2.4%, 0.4% ± 3.1%, - 0.9% ± 4.0%, - 0.8% ± 1.1%, and - 0.5% ± 2.0%, respectively, and correlation coefficients of r = 0.99 for all. In all patients, there was no difference in the management decision of whether or not to stop PRRT because of unsafe absorbed dose to risk organs using either the standard protocol or the (t1, t3) protocol.
Conclusion: These preliminary results demonstrate that dosimetry calculations using two quantitative SPECT/CT studies acquired at 24 and 168 h after the first PRRT cycle are feasible and are in good agreement with the standard imaging protocol with no change in patient management decisions, while enabling improved patient comfort and reduced scanner and staff time.
Keywords: Dosimetry; Peptide receptor radionuclide therapy (PRRT); SPECT/CT; [177Lu]-DOTA-TATE.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Kwekkeboom DJ, de Herder WW, Kam BL, van Eijck CH, van Essen M, Kooij PP, et al. Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol Off J Am Soc Clin Oncol. 2008;26:2124–2130. - PubMed
-
- Bodei L, Cremonesi M, Grana CM, Fazio N, Iodice S, Baio SM, et al. Peptide receptor radionuclide therapy with 177Lu-DOTATATE: the IEO phase I-II study. Eur J Nucl Med Mol Imaging. 2011;38:2125–2135. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
