

doi: 10.2337/cd20-as01.
Standards of Medical Care in Diabetes-2020 Abridged for Primary Care Providers
- PMID: 31975748
- PMCID: PMC6969656
- DOI: 10.2337/cd20-as01
Item in Clipboard
Standards of Medical Care in Diabetes-2020 Abridged for Primary Care Providers
Clin Diabetes.
2020 Jan.
No abstract available
Figures
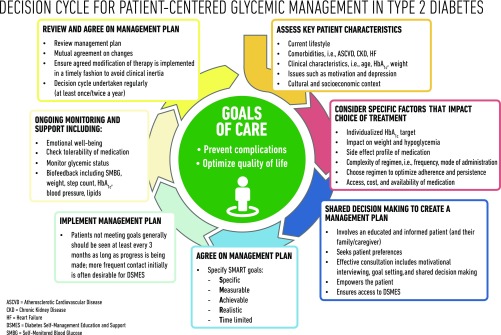
Decision cycle for patient-centered glycemic management in type 2 diabetes. HbA1c, glycated hemoglobin. Reprinted from Davies MJ, D’Alessio DA, Fradkin J, et al. Diabetes Care 2018;41:2669–2701.
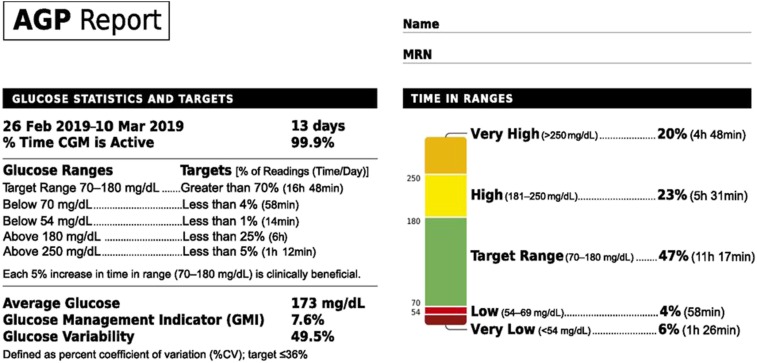
Sample AGP report. Adapted from Battelino T, Danne T, Bergenstal RM, et al. Diabetes Care 2019;42:1593–1603.
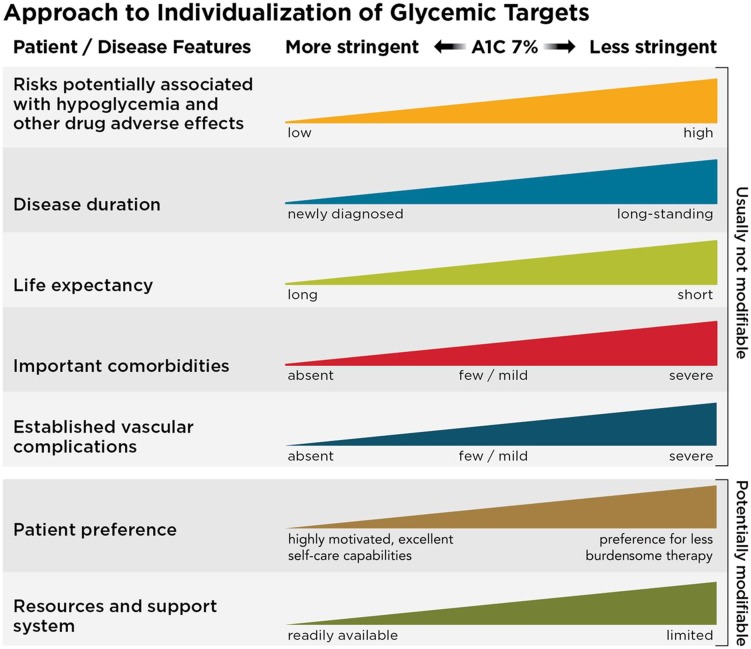
Depicted are patient and disease factors used to determine optimal A1C targets. Characteristics and predicaments toward the left justify more stringent efforts to lower A1C; those toward the right suggest less stringent efforts. A1C 7%553 mmol/mol. Adapted with permission from Inzucchi SE, Bergenstal RM, Buse JB, et al. Diabetes Care 2015;38:140–149.
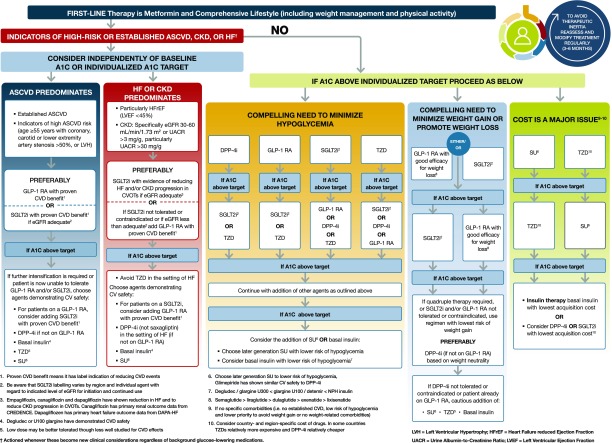
Glucose-lowering medication in type 2 diabetes: overall approach. For appropriate context, see Figure 4.1. CREDENCE, Evaluation of the Effects of Canagliflozin on Renal and Cardiovascular Outcomes in Participants With Diabetic Nephropathy. CVOTs, CV outcomes trials; DPP-4i, dipeptidyl peptidase 4 inhibitor; GLP-1 RA, GLP-1 receptor agonist; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea; TZD, thiazolidinedione. Adapted from Davies MJ, D'Alessio DA, Fradkin J, et al. Diabetes Care 2018;41:2669–2701 and Buse JB, Wexler DJ, Tsapas A, et al. Diabetes Care 19 December 2019 [Epub ahead of print]. DOI: 10.2337/dci19-0066.
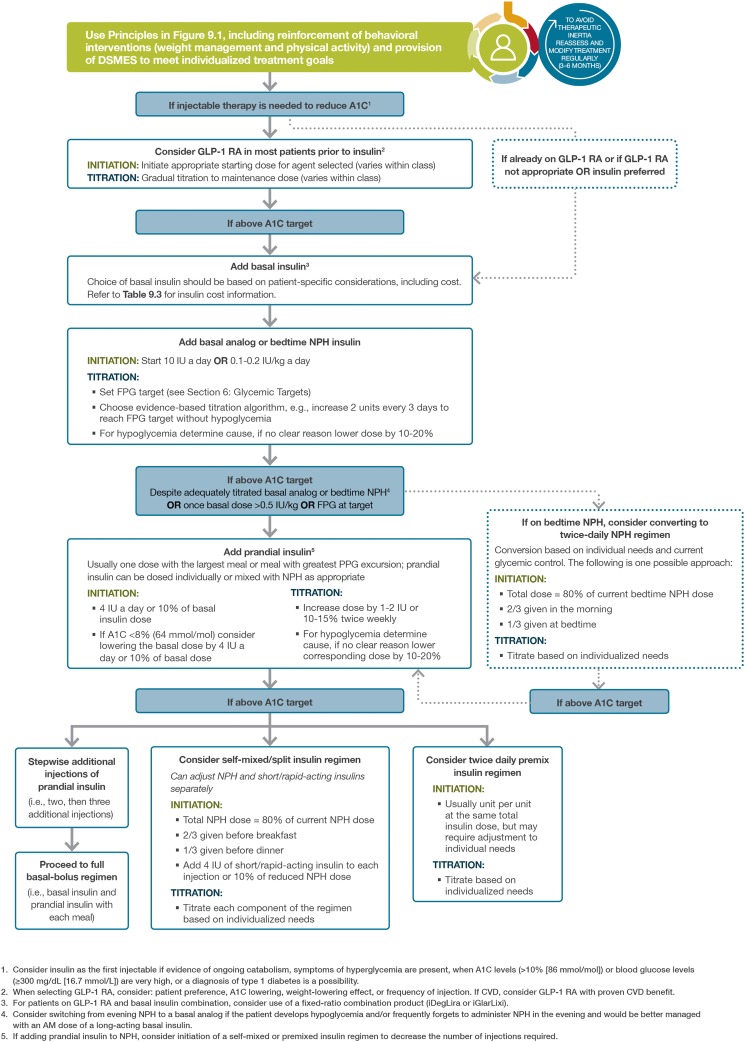
Intensifying to injectable therapies. FPG, fasting plasma glucose; FRC, fixed-ratio combination; GLP-1 RA, GLP-1 receptor agonist; iDegLira, insulin degludec/liraglutide; iGlarLixi, insulin glargine/lixisenatide; max, maximum; PPG, postprandial glucose; Table 9.3 appears in the complete 2020 Standards of Care. Adapted from Davies MJ, D'Alessio DA, Fradkin J, et al. Diabetes Care 2018;41:2669–2701.
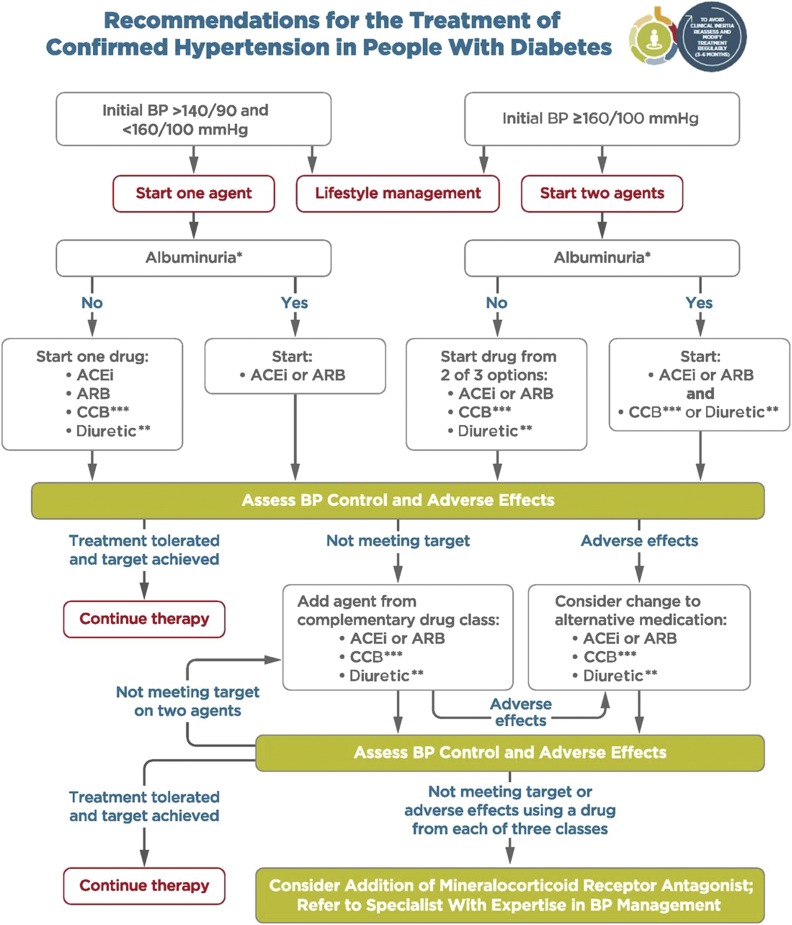
Recommendations for the treatment of confirmed hypertension in people with diabetes. *An ACE inhibitor (ACEi) or ARB is suggested to treat hypertension for patients with a UACR 30–299 mg/g Cr and strongly recommended for patients with a UACR ≥300 mg/g Cr. **Thiazide-like diuretic; long-acting agents shown to reduce CV events, such as chlorthalidone and indapamide, are preferred. ***Dihydropyridine CCB. BP, blood pressure. Adapted from de Boer IH, Bangalore S, Benetos A, et al. Diabetes Care 2017;40:1273–1284.
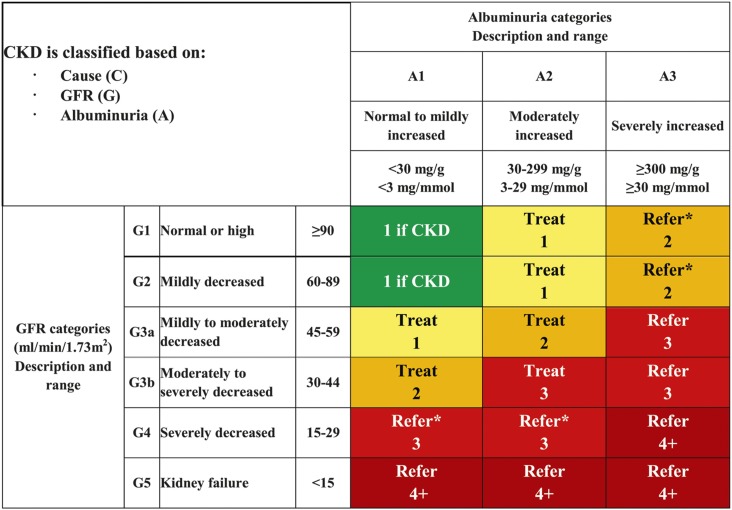
Risk of CKD progression, frequency of visits, and referral to nephrology according to GFR and albuminuria. The GFR and albuminuria grid depicts the risk of progression, morbidity, and mortality by color, from best to worst (green, yellow, orange, red, dark red). The numbers in the boxes are a guide to the frequency of visits (number of times per year). Green can reflect CKD with normal eGFR and UACR only in the presence of other markers of kidney damage, such as imaging showing polycystic kidney disease or kidney biopsy abnormalities, with follow-up measurements annually; yellow requires caution and measurements at least once per year; orange requires measurements twice per year; red requires measurements three times per year; and dark red requires measurements four times per year. These are general parameters only, based on expert opinion, and underlying comorbid conditions and disease state as well as the likelihood of impacting a change in management for any individual patient must be taken into account. “Refer” indicates that nephrology services are recommended. *Referring clinicians may wish to discuss with their nephrology service, depending on local arrangements regarding treating or referring. Reprinted with permission from Vassalotti JA, Centor R, Turner BJ, Greer RC, Choi M, Sequist TD; National Kidney Foundation Kidney Disease Outcomes Quality Initiative. Am J Med 2016;129:153–162.e7.
LinkOut - more resources
Full Text Sources
Other Literature Sources
